Associate Professor of Pediatrics University of Wisconsin Madison, Wisconsin, United States
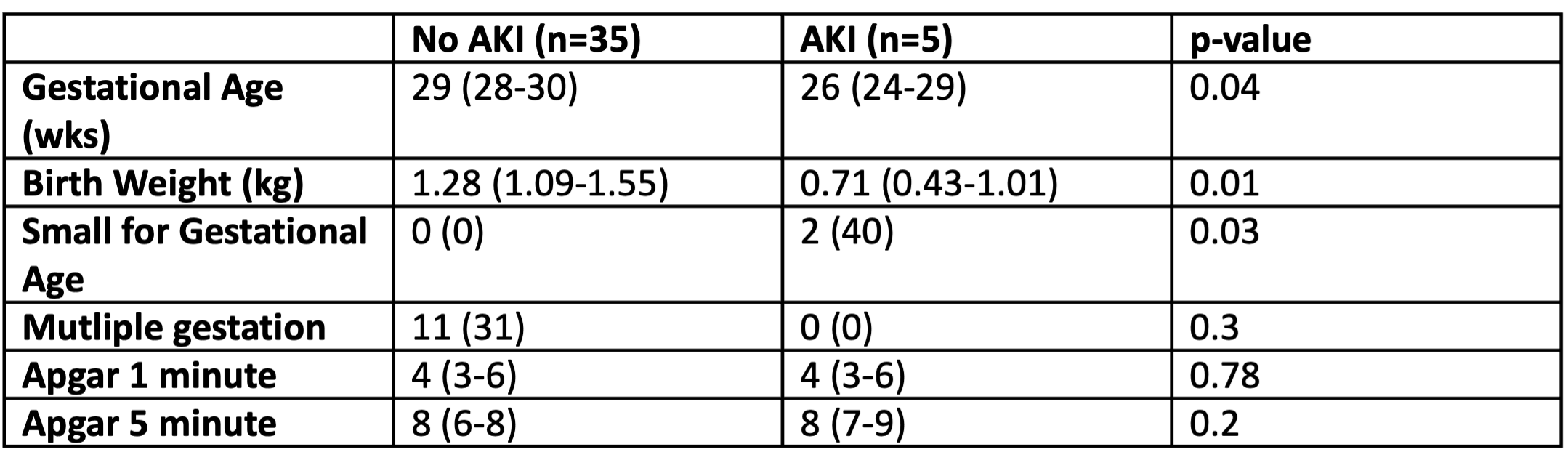
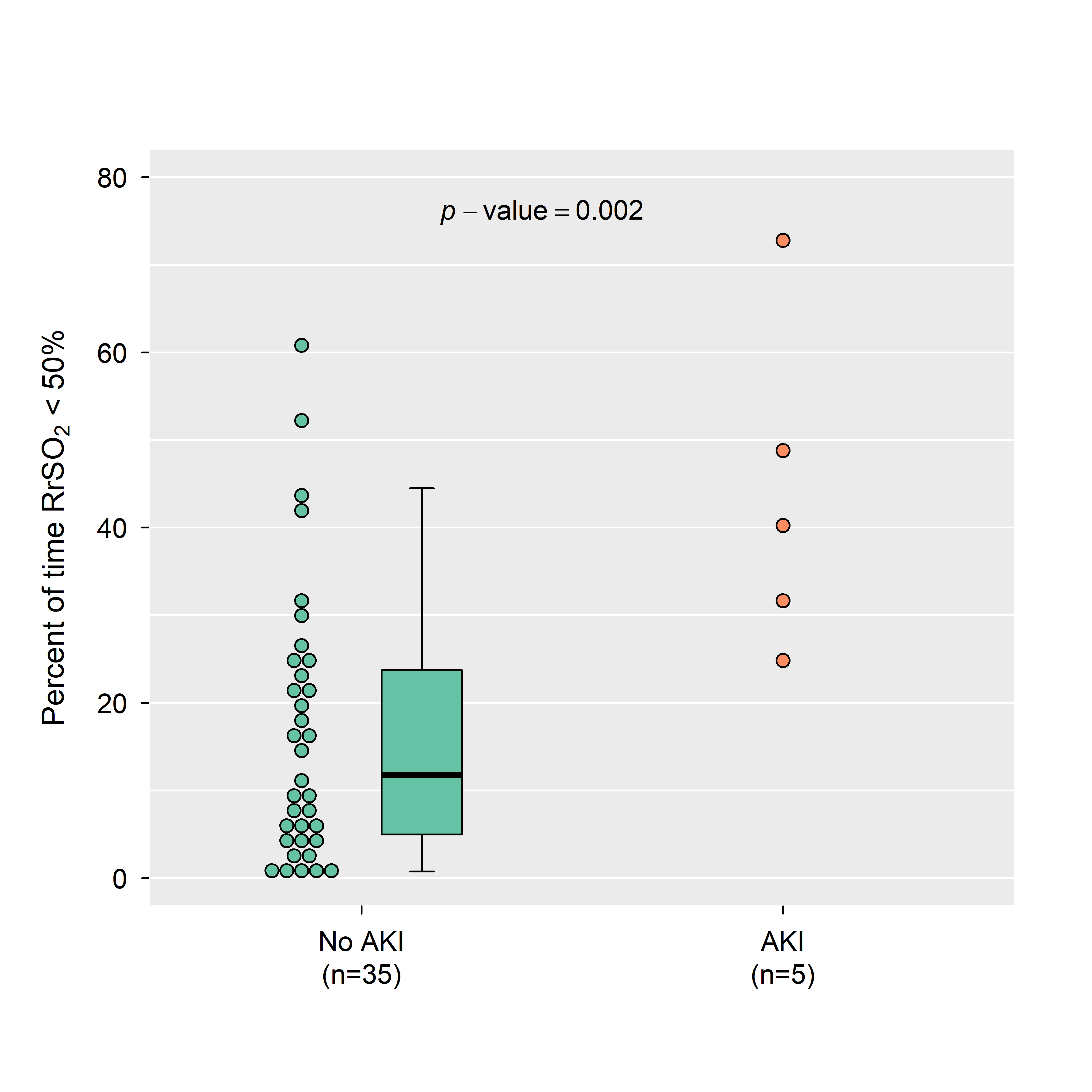
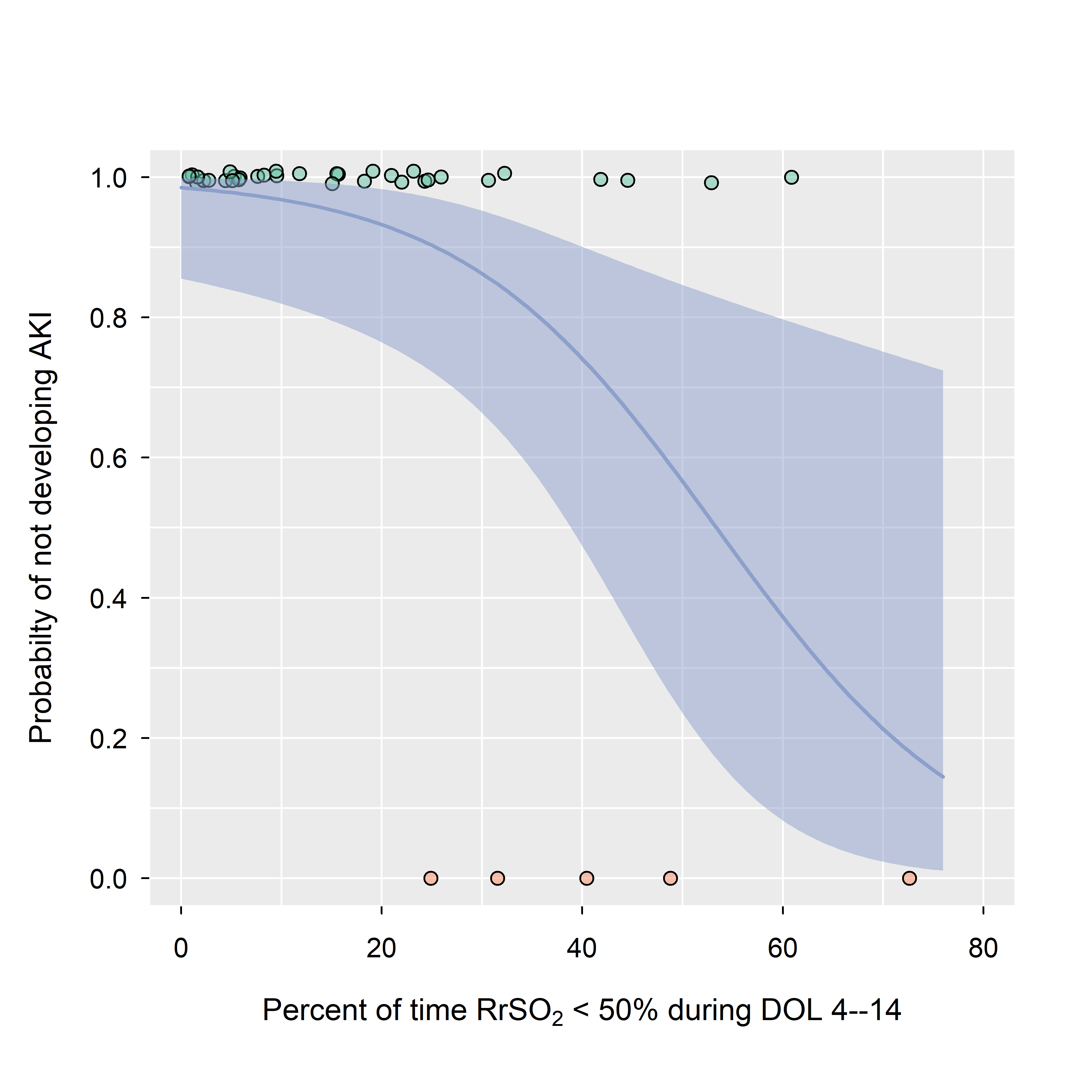
Background: Changes in urine output and serum creatinine (SCr) used to diagnose acute kidney injury (AKI) are temporally delayed, preventing changes in care or therapeutic intervention. Monitoring kidney oxygenation continuously and non-invasively with near infrared spectroscopy (NIRS) is safe and feasible in preterm neonates. Previous studies have demonstrated normal oxygenation as >50%. However, the correlation between kidney hypoxia < 50% and AKI is unknown. Objective: To compare kidney oxygenation in preterm neonates with and without AKI. Design/Methods: A prospective observational study of preterm neonates born at < 32 weeks gestational age with Invos NIRS 5100C monitors and neonatal sensors was performed from 2021-2022. Sensors were applied by 4 days of age and continued through 14 days of age. Every 6-hour urine output and all clinically obtained SCr values were collected via chart review. Participants were staged for AKI using the modified neonatal KDIGO definition. Each participant’s kidney oxygenation was summarized by noting the proportion of time < 50%. For infants who developed AKI, the proportion was calculated over the interval of time prior to AKI onset. Logistic regression was used to estimate odds of not having AKI as a function of the fraction of time < 50%. Results: 40 participants with median birth weight 1.25 kg (IQR 1.02-1.45) and gestational age of 29 weeks (IQR 27-30) were included (Table 1). Time spent below the 50% cut-off decreases with increasing birth weight (Spearman's correlation = -0.52, p < 0.001). Five participants developed AKI, four with stage 1 injury and one with stage 2 injury. Participants with AKI spent significantly more time with values < 50% compared to those without AKI (Figure 1, 41.3% vs. 12.4% respectively, p=0.002). Given one infant with AKI and one without, there’s an estimated 89.7% chance the one with AKI had a larger proportion of time < 50% compared to an infant without AKI (95% CI: 74.1–96.4%). If the kidney oxygenation remains < 50% for at most 25.4% of the time, the probability of not having AKI is at least 90% (Figure 2, one-sided 95% CI: at most 38.3%).
Conclusion(s): Preterm neonates with clinical AKI have significantly more kidney hypoxia than those with no AKI in the first two weeks of life. Larger multisite trials are needed to increase the sample size of participants with AKI to validate these findings.

 photo")