Assistant Professor of Pediatrics, Division of Neonatology Medical College of Wisconsin Milwaukee, Wisconsin, United States
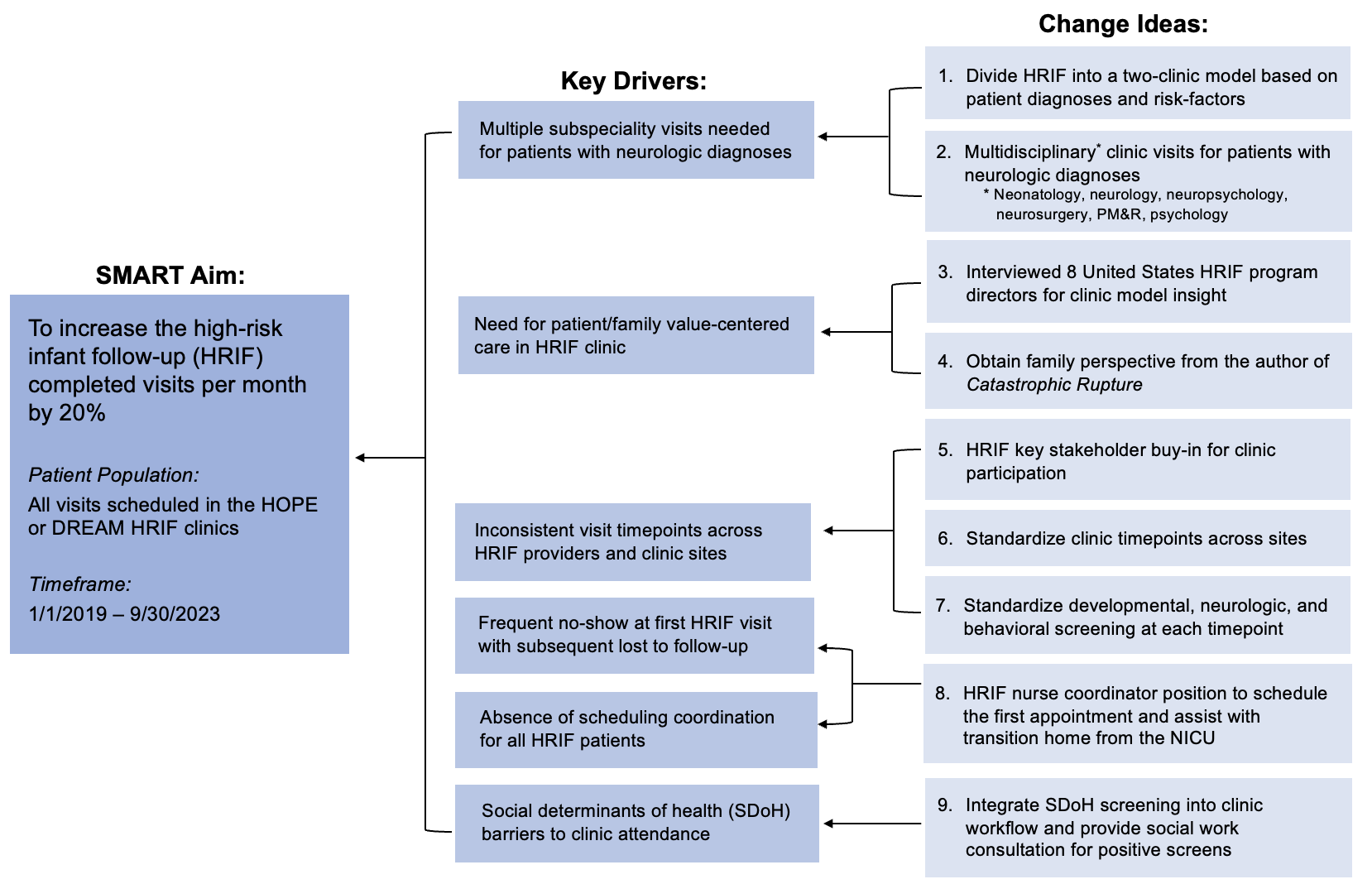
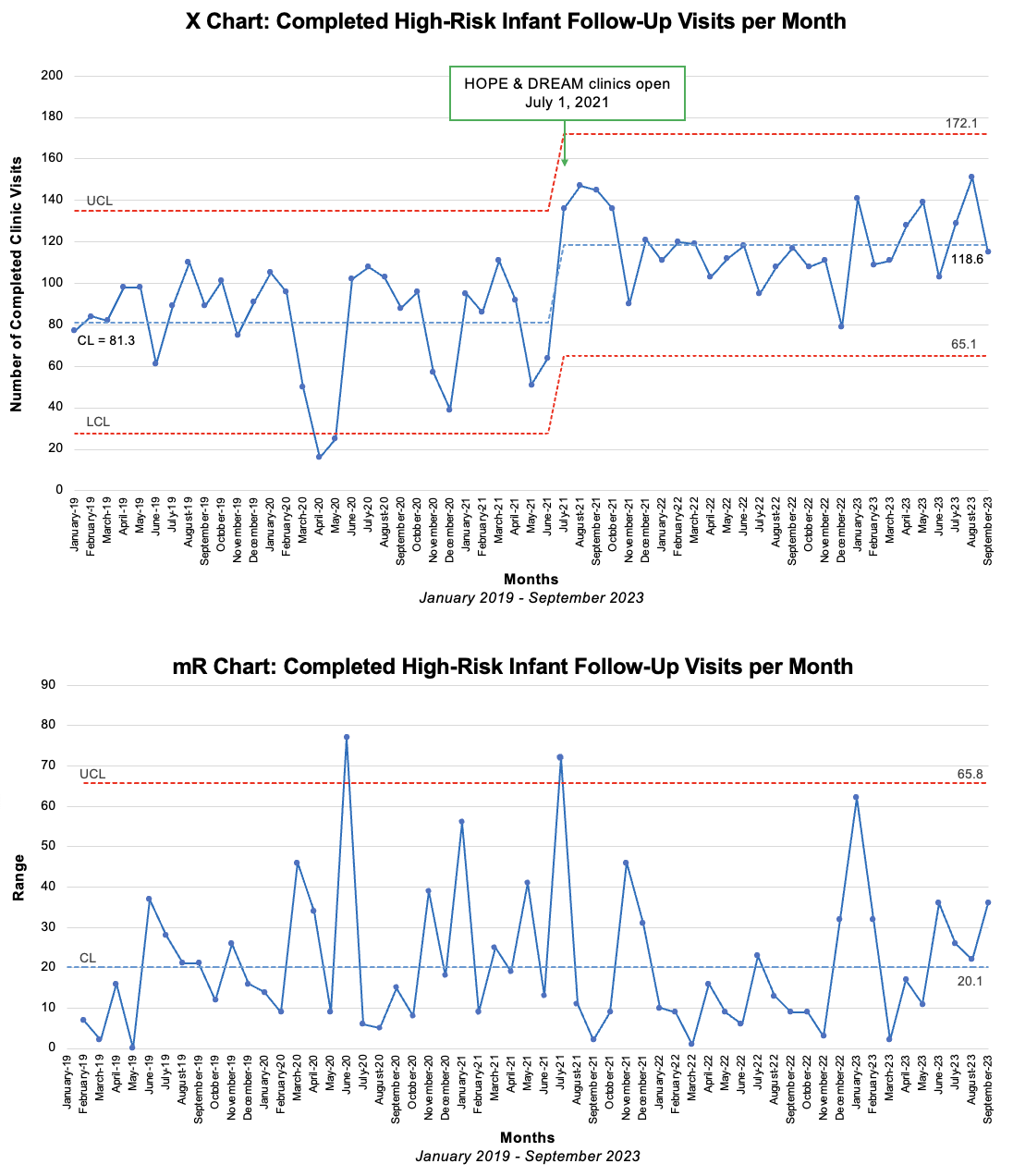
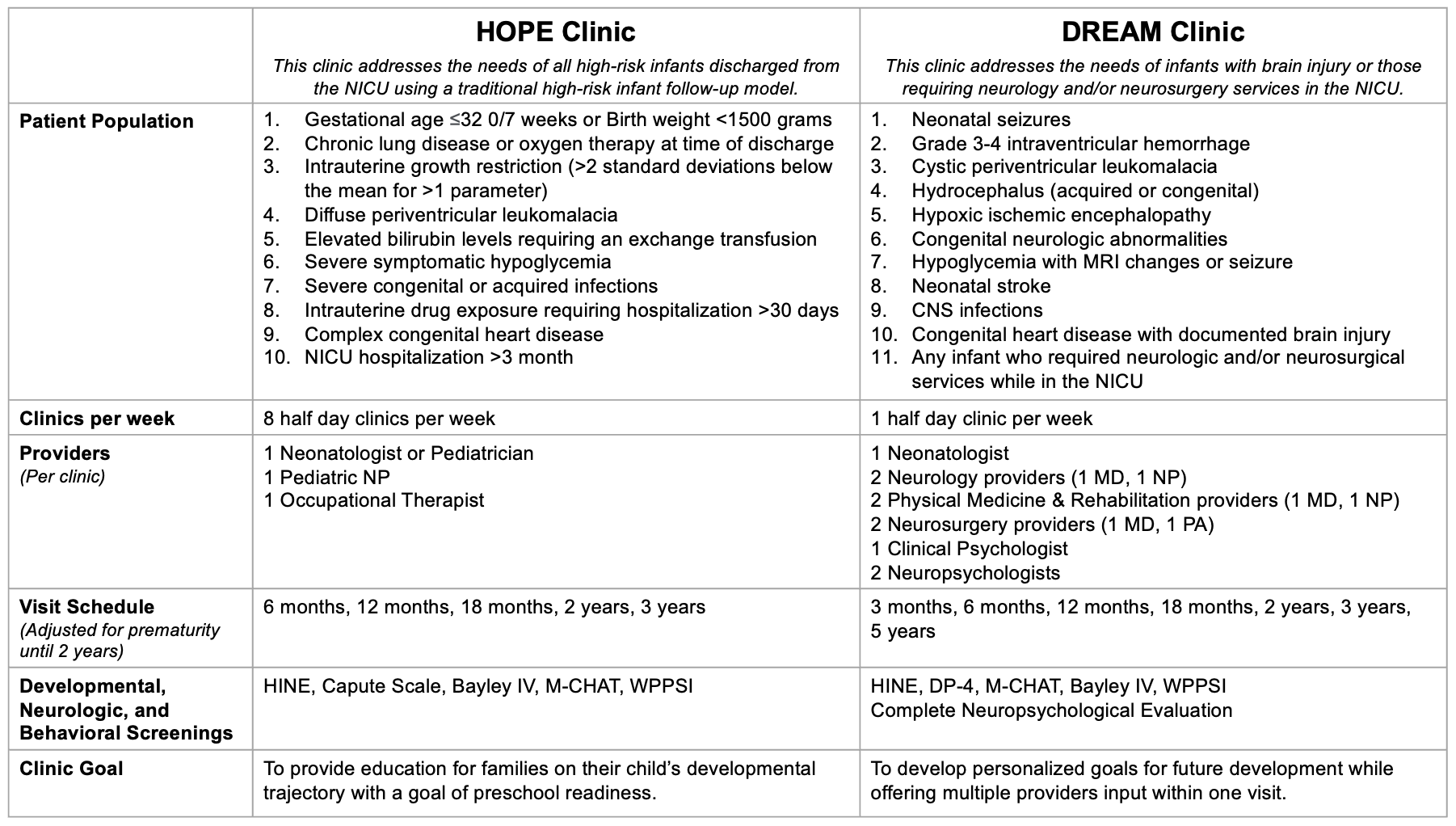
Background: High-risk infant follow-up (HRIF) programs must provide developmental assessments of NICU graduates with complex diagnoses beyond prematurity. Despite known benefits of HRIF, sustained clinic attendance remains challenging. To address the developmental needs of this diverse population, improved HRIF clinic participation is necessary. Objective: We aimed to increase the number of completed HRIF visits per month by 20% between 1/1/2019 and 9/30/2023 using a novel two-clinic model. Design/Methods: We conducted a multidisciplinary quality improvement (QI) project in our level IV NICU and HRIF clinic. A key driver diagram was constructed to determine the drivers and change ideas (Figure 1). Implementation of a two-clinic model (HOPE & DREAM clinics) served as our primary intervention (Table 1). This model risk-stratifies infants by diagnosis to provide personalized developmental care. Change ideas also included NICU provider and family education, scheduling coordination, social determinants of health (SDoH) screening, and a focus on value-centered care. The outcome measure was the number of completed HRIF visits per month. The process measure was the percent of HRIF visit no-shows per month. Balancing measures were primary care provider satisfaction and perceived family experience obtained by anonymous surveys using a Likert scale before and after the primary intervention. Statistical process control charts were used to assess the intervention impact. Results: Prior to implementation of the two-clinic model, a mean of 81.3 HRIF visits were completed per month. After the primary intervention on 7/1/2021, completed visits increased by 46% to a mean of 118.6 visits per month (Figure 2). Special cause variation was achieved and sustained through 9/30/2023. The percent visit no-shows per month decreased from 14% to 10%. Percent of primary care providers satisfied with the HRIF program remained unchanged at 96% and perceived family satisfaction increased from 64% to 75% after the intervention.
Conclusion(s): Through the HOPE & DREAM clinic model, we exceeded our clinic attendance goal without compromising primary care provider and family satisfaction. We speculate that this improvement resulted from culture change surrounding the value of HRIF. Our next step is to measure and improve patient retention over time.

 photo")