Medical Student Southern Illinois University School of Medicine Springfield, Illinois, United States
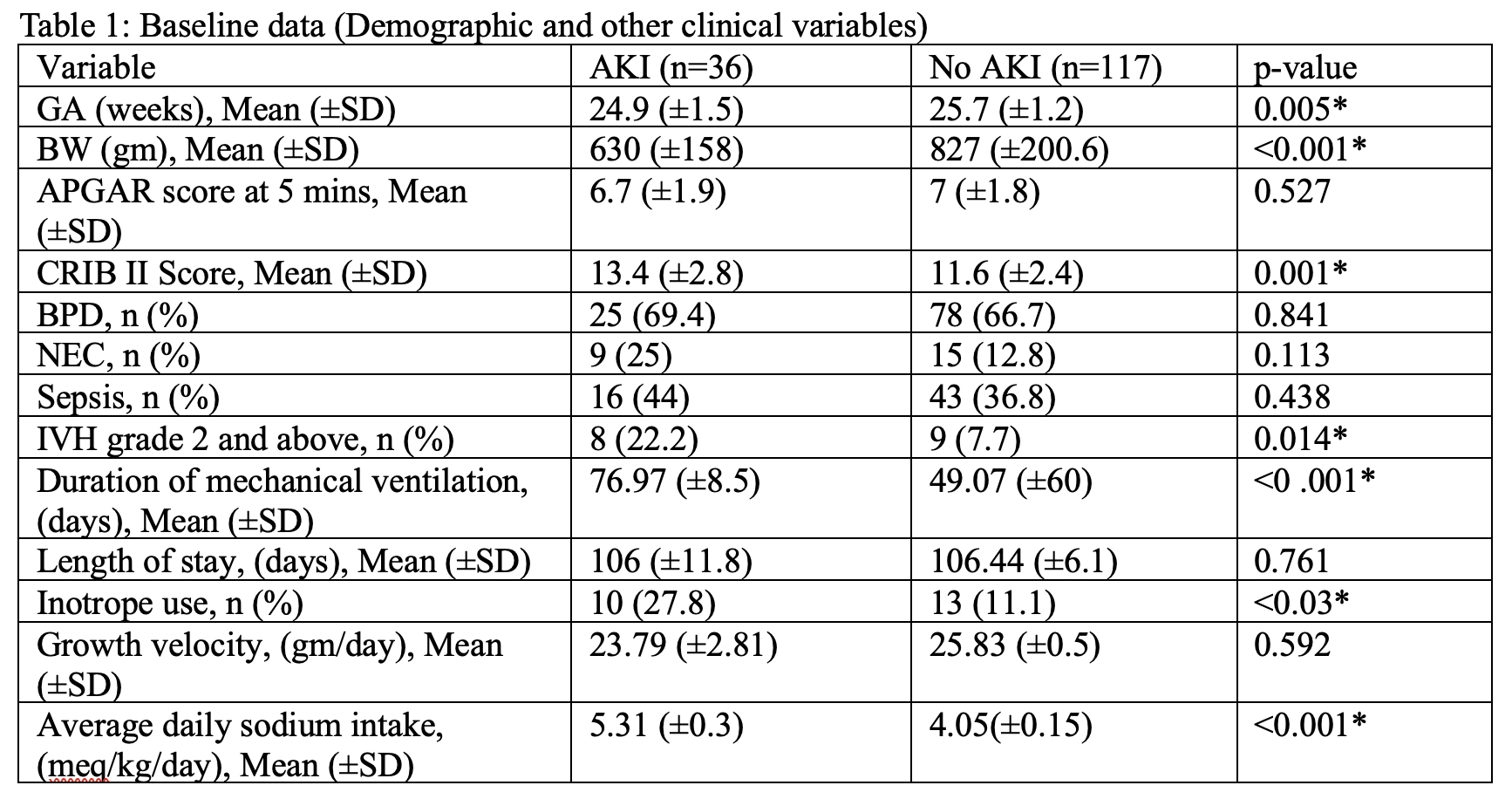
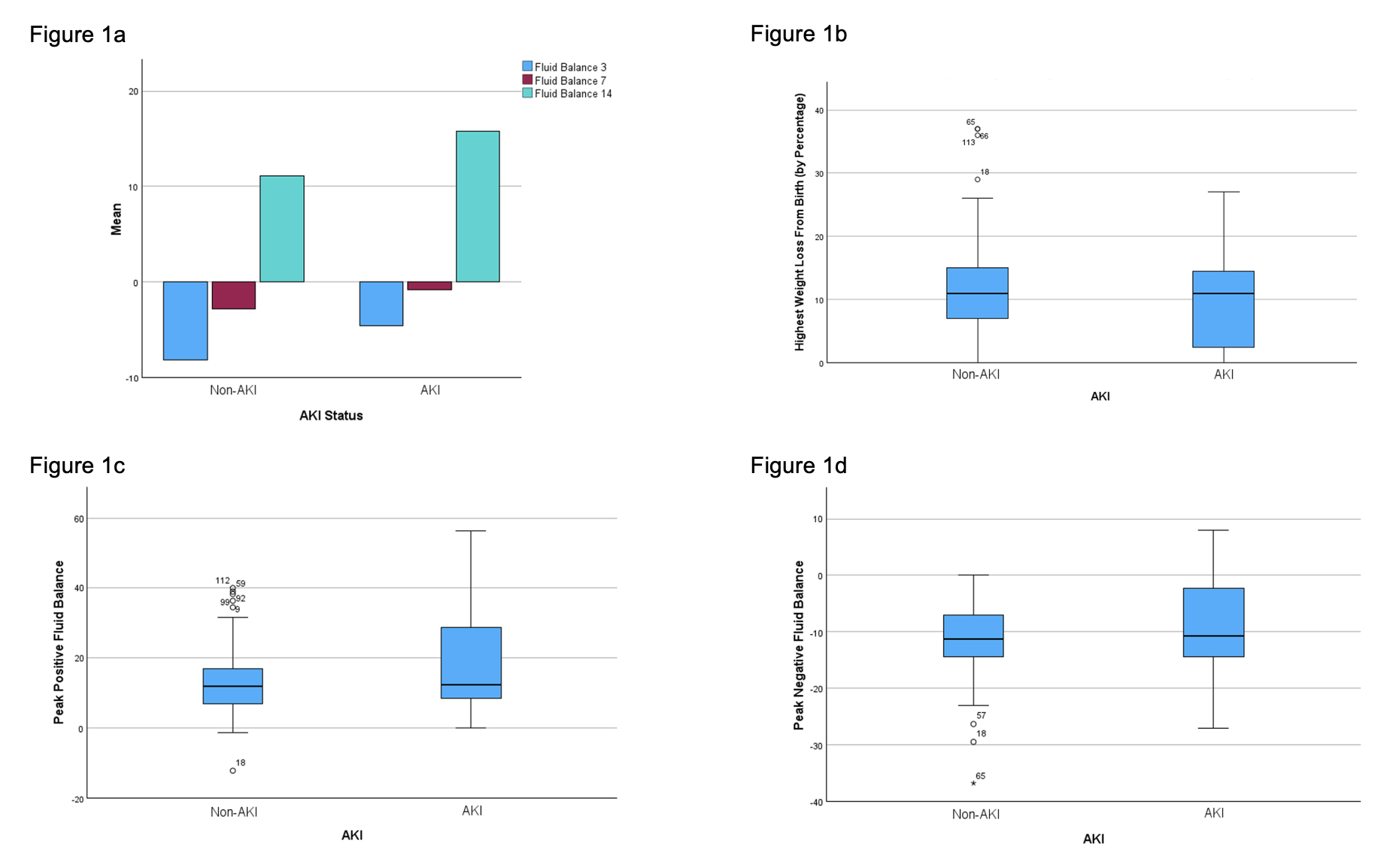
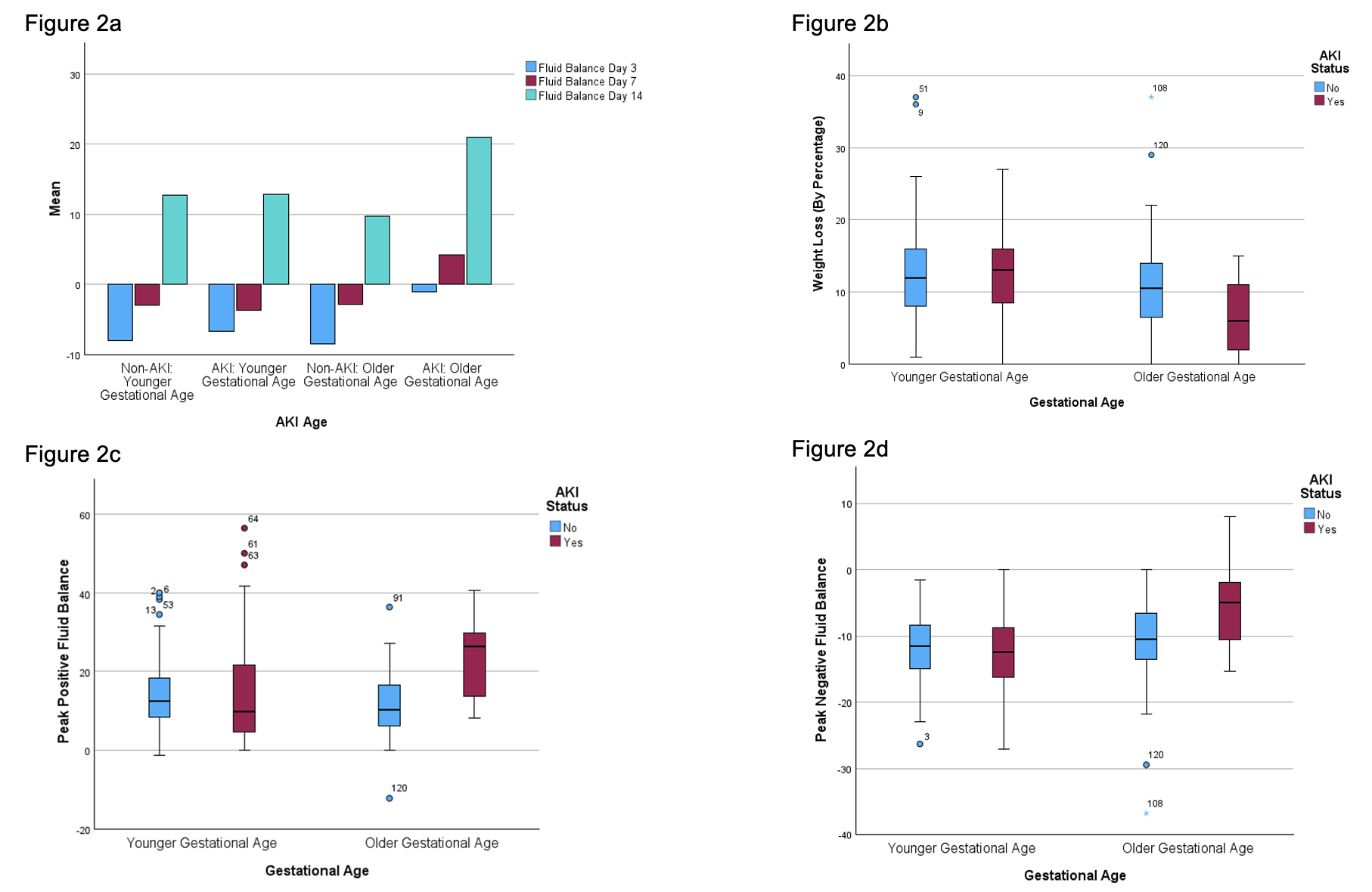
Background: Extremely low gestational age neonates (ELGAN) are at increased risk of acute kidney injury (AKI) which is associated with increased mortality and poor outcomes. Volume depletion has been implicated as a cause for AKI with fluid overload occurring consequently. However, the degree of fluid overload in infants with AKI and the impact of fluid balance (FB) in the development of AKI in ELGAN has not been studied. Objective: To explore factors associated with AKI, evaluate the impact of FB in the first 14 postnatal days on the development of AKI, and determine the impact of AKI on the growth velocity in ELGAN. Design/Methods: Retrospective cohort study of all ELGAN (230/7-276/7 weeks GA) at a level III NICU (ADC 40, >700 annual admissions) over a 5-year period (4/2018-3/2023). Infants with and without AKI were classified based on neonatal modified KDIGO definition of AKI. Data analyzed included demographics, clinical variables, in-hospital outcomes, growth velocity, fluid and sodium intake, and weight change during the first 14 post-natal days. FB was calculated as [(Daily Weight − Birth Weight) / Birth Weight] × 100. Peak positive and negative FB during first 14 days, and FB on day 3, 7, and 14 were compared between the two groups. The infants were stratified based on GA as younger GA (23-25 wks) and older GA (26-27 wks). Data was analyzed using appropriate statistical tests and p < 0.05 was considered significant. Results: 36 neonates with AKI were compared to 117 neonates without AKI. When compared to controls, infants with AKI are found to be less mature, have lower BW and higher CRIB II scores, and are more likely to develop IVH, require prolonged mechanical ventilation, and utilize inotropes (Table 1). Other demographic and clinical variables between the two groups were similar. FB on day 3, 7, and 14, as well as the peak positive and negative FB were similar between the two groups (Figure 1). Infants with older GA had lower peak negative (4.9% vs 10.4%, p = 0.01) and higher peak positive FB (26.5% vs 10.4%, p < 0.001) in the AKI group (Figure 2). Additionally, patients with AKI had a greater average daily sodium intake (Table 1). The growth velocity was similar between the two groups (p=0.59).
Conclusion(s): Infants with AKI are less mature, sicker at birth, and more likely to have IVH. They require more inotropic support and prolonged mechanical ventilation. ELGAN with older GA also tend to have higher positive fluid balance. Further investigation in a larger prospective study may help clarify why this only occurs in infants of older GA.

.jpg "Lauren R. Kee (she/her/hers) photo")