Resident Cincinnati Children's Hospital Medical Center Cincinnati, Ohio, United States
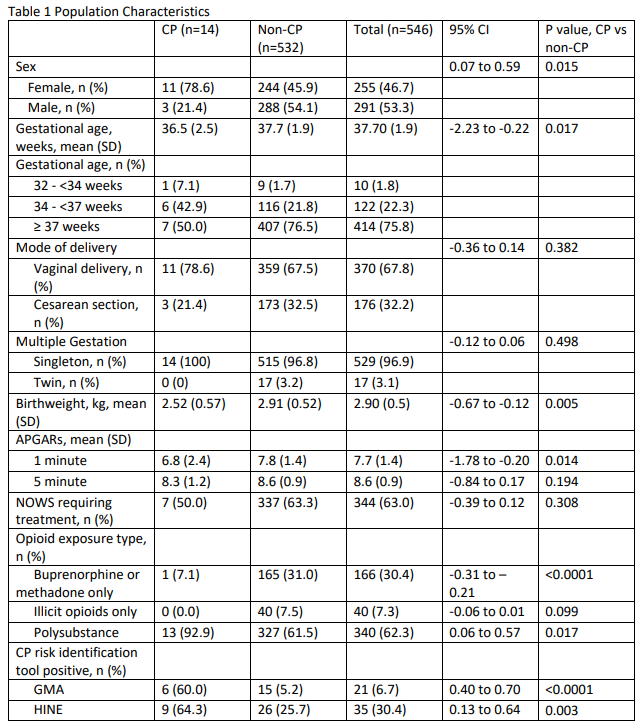
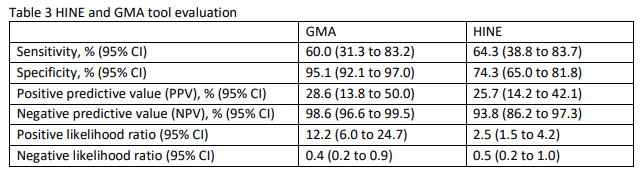
Background: Opioid use during pregnancy and the rate of neonatal opioid withdrawal syndrome (NOWS) have increased in recent years. There are known adverse cognitive and behavioral outcomes associated with prenatal opioid exposure, but there is relatively little information regarding motor outcomes including cerebral palsy (CP). The General Movements Assessment (GMA) and Hammersmith Infant Neurological Examination (HINE) are tools to identify infants at risk for CP and other neurologic abnormalities; however, there is limited data on the use of these tools in the specific population of infants with prenatal opioid exposure. CP rates vary by gestational age, though the average incidence is estimated to be between 1.5 to 3 per 1,000 births (0.15% to 0.3%). Objective: To determine CP rates in children with prenatal opioid exposure seen in NOWS clinic. To determine the utility of the GMA and HINE as tools to identify CP in the NOWS population. Design/Methods: Retrospective cohort study of 546 opioid-exposed infants born between 1/1/2020 and 10/1/2022 that were seen in NOWS Follow-Up Clinic. Infants with neonatal detectable CP risk factors (including prematurity < 32 weeks) were excluded. Our primary outcome was CP diagnosis. Our secondary outcome was rate of abnormal GMA and HINE between the CP and non-CP groups. Other factors examined include sex, mode of delivery, gestational age, APGARs at 1 and 5 minutes, NOWS requiring treatment, and type of opioid exposure. Unpaired t-test was used to compare the means of CP and non-CP groups. Results: Fourteen of the 546 opioid-exposed infants (2.6%) were diagnosed with CP at time of data analysis. Sixty percent of those later diagnosed with CP had an absent fidgety GMA and 64% had HINE below the cutoff, whereas 5% of those without a CP diagnosis had an absent fidgety GMA and 26% had a HINE below the cutoff. The GMA and HINE had negative predictive values of nearly 99% and 94%, respectively. The odds ratio for CP in infants with polysubstance exposure (defined as multiple opioid or illicit drug exposure) was 8.15 compared to those without polysubstance exposure.
Conclusion(s): CP rates in opioid exposed infants seen in NOWS clinic are significantly higher than in the general population. The GMA and HINE may be helpful tools to identify infants at high risk for CP in the NOWS population, as they are in other populations. Our data suggests that prenatal polysubstance exposure may be associated with higher rates of CP than medication-assisted treatment exposures (buprenorphine or methadone) or single illicit opioid exposure.

 photo")