Medical Student Southern Illinois University School of Medicine Springfield, Illinois, United States
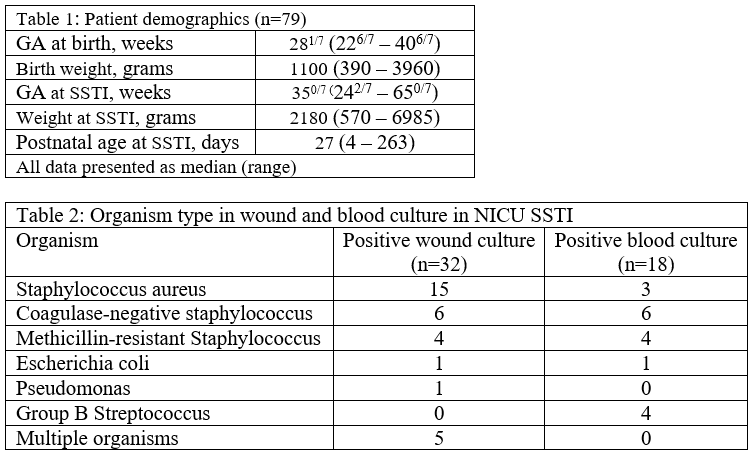
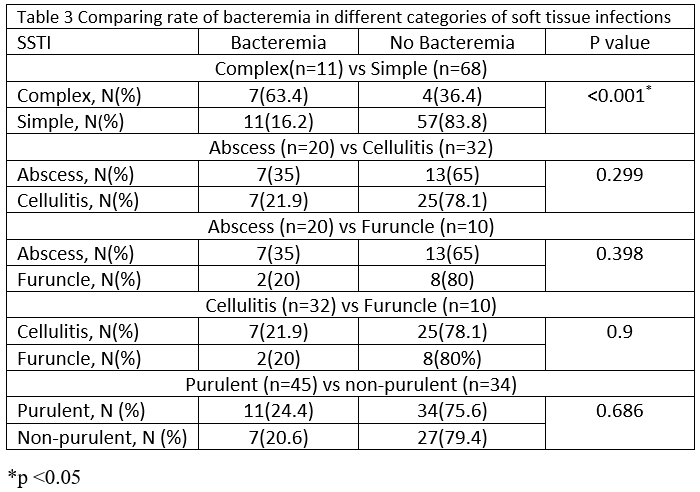
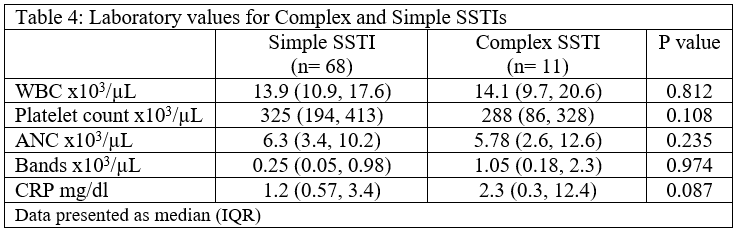
Background: Skin and soft tissue infections (SSTI) are mostly caused by Staphylococcus aureus. SSTIs are classified as non-purulent and purulent. Mild purulent soft tissue infections/abscesses are often managed only with incision and drainage in older children and adults. Bacteremia is rare in afebrile infants with SSTI. In our hospital, we have a clinical pathway for the management of SSTI in children, but infants less than 2 months of age are excluded as there is a paucity of data on neonates with SSTI. Objective: To determine the correlation of types of SSTI with bacteremia and laboratory parameters in neonates in the NICU. Design/Methods: Retrospective study on all patients who underwent late-onset sepsis (LOS) evaluations and had evidence of an SSTI from 01/2012 – 04/2023 at a level III NICU (ADC: 40, >700 annual admissions). SSTIs were categorized as non-purulent (cellulitis, erysipelas, and necrotizing infection) and purulent (furuncles, carbuncles, and abscesses) and based on severity as complex and simple. Demographic, clinical, and laboratory characteristics were analyzed, and rates of bacteremia were compared between different categories of SSTI. Lab values between simple and complex SSTI were also compared. The chi-square test and the Mann-Whitney U test were used to determine statistical significance (p < 0.05). Results: 79(1%) SSTI out of 7405 NICU admissions were identified. SSTIs included abscesses (n=20), cellulitis (n=32), furuncle (n=10), and other purulent infections (n=17). Demographics for SSTI patients are in Table 1. Iatrogenic SSTI (n=39, 49%) was associated with an IV site (n=19), surgical incision (n=12), and gastrostomy tube site (n=8). Organisms identified from wound culture [n=32/37] and neonates with bacteremia [n=18/79]) are listed in Table 2. As shown in table 3, bacteremia was significantly more with complex SSTI (7/11, 63.4%) vs simple SSTIs (11/68, 16.2%; p< 0.001) but the incidence of bacteremia was similar between other categories of SSTI purulent vs non-purulent (24.4% vs 20.6%, p=0.686), abscess vs cellulitis (35% vs 21.9%, p=0.229), abscess vs furuncle (35% vs 20.6%, p=0.398), and cellulitis vs furuncle (21.9% vs 20.6%, p=0.9). Lab values did not differ between complex and simple SSTIs (Table 4).
Conclusion(s): Over an 11-year period, the incidence of SSTI was low in a cohort of >7000 NICU patients. Bacteremia was more common for complex SSTI when compared to simple SSTI, but otherwise similar across various types of SSTIs. Despite higher bacteremia rate in complex SSTI, lab values did not differ from simple SSTI.

 photo")