Resident University of Alabama School of Medicine Birmingham, Alabama, United States
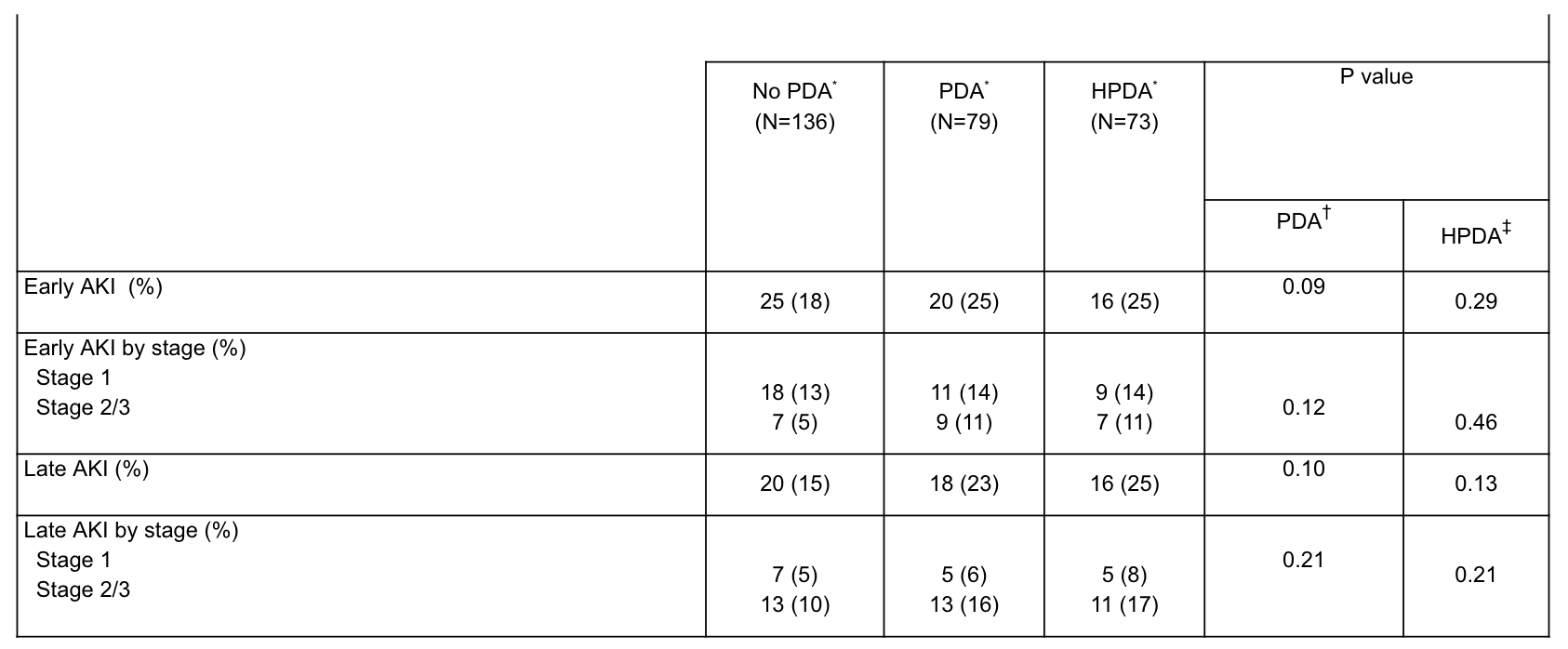
Background: Given the growing evidence supporting therapeutic abstention for the management of patent ductus arteriosus (PDA) early in hospitalization, preterm infants may be exposed to a PDA for prolonged periods of time. Acute kidney injury (AKI) has previously been associated with PDA exposure, although the association between prolonged PDA exposure and AKI has not previously been described. Objective: We hypothesized that the duration of PDA and hemodynamically significant PDA (HPDA) exposure would be associated with (1) risk for AKI (2) frequency of AKI events, and (3) severity of AKI. Design/Methods: Retrospective case-control study among preterm infants from 22w 0d to 28w 6d born between 2017 and 2020, hospitalized at the University of Alabama at Birmingham, and who remained on respiratory support on postnatal day 28. Infants that developed evidence of AKI by Kidney Disease Improving Global Outcomes criteria (cases) were compared to infants that did not develop AKI (controls). Acute kidney injury was further stratified by severity and the postnatal age at which AKI occurred with early AKI defined as occurring up to and including postnatal day 28 and late AKI occurring after postnatal day 28. Data from all echocardiograms performed during the hospitalization after 28 weeks’ post-menstrual age (PMA) were included so as to define the duration of PDA exposure related to study outcomes. Descriptive comparisons between AKI and AKI severity by PDA and HPDA status were analyzed using Fisher’s exact test. Results: Two hundred fifteen infants were included over the 4-year period, of whom 45 (21%) of infants developed early AKI and 38 (18%) developed late AKI. No statistically significant difference was observed for early AKI with a PDA (p=0.09) or HPDA (p=0.29) or for infants with late AKI that had a PDA (p=0.10) or HPDA (0.13)(Table 1). Infants with longer durations of HPDA exposure for 12 weeks had an increased risk for stage 2/3 AKI compared to infants without a PDA on postnatal day 28 (risk ratio 2.75; 95% CI 1.19-6.39).
Conclusion(s): In this observational study in infants on respiratory support on postnatal day 28, the frequency of early and late AKI did not differ by PDA status and hemodynamic significance. However, more prolonged periods of HPDA exposure were associated with higher frequency of severe AKI compared to infants with no PDA.

 photo")