411 - A Systematic Review and Meta-analysis Comparing Ultrasound versus Radiology in reducing the incidence of Central Catheter related complications in Neonates.
Associate professor University of Toronto Temerty Faculty of Medicine Toronto, Ontario, Canada
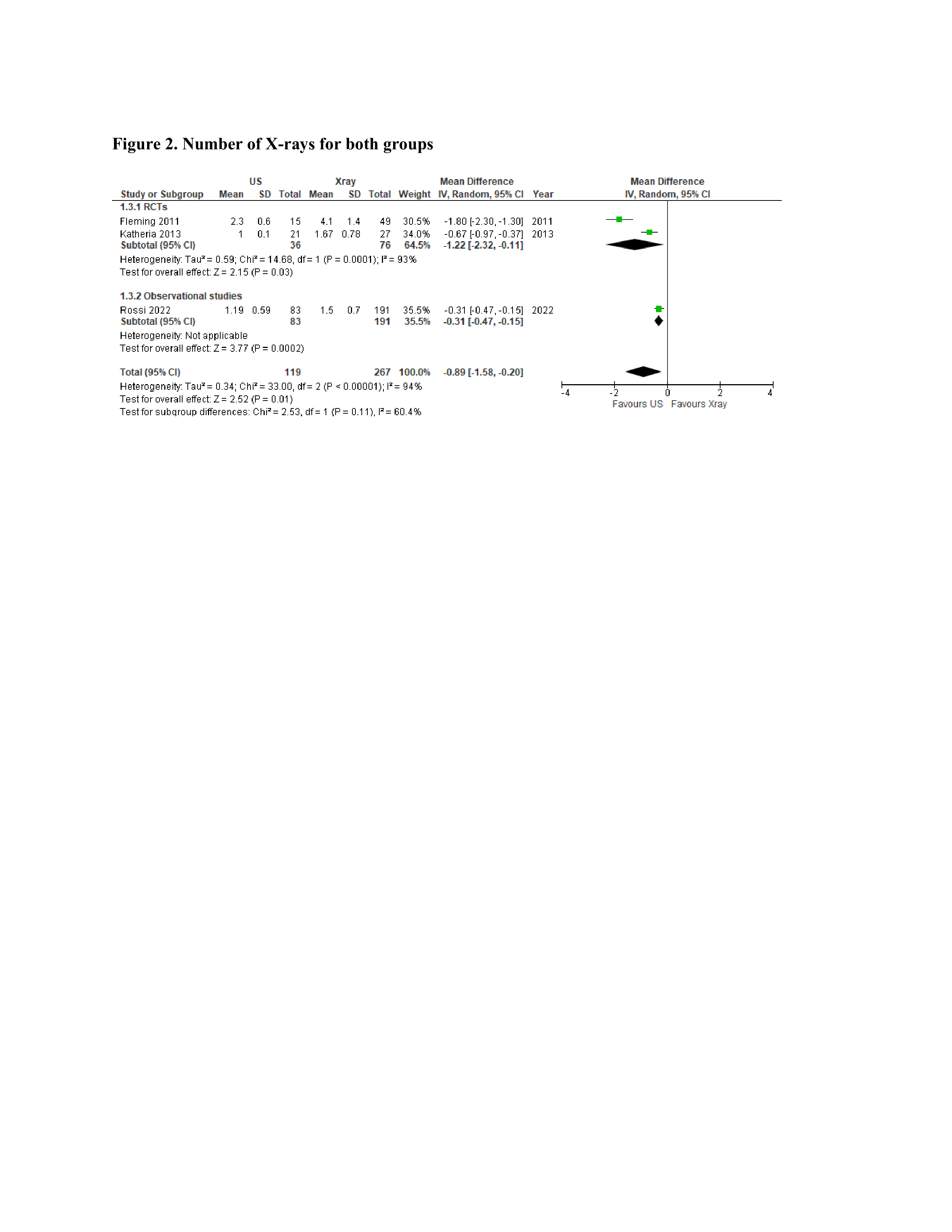
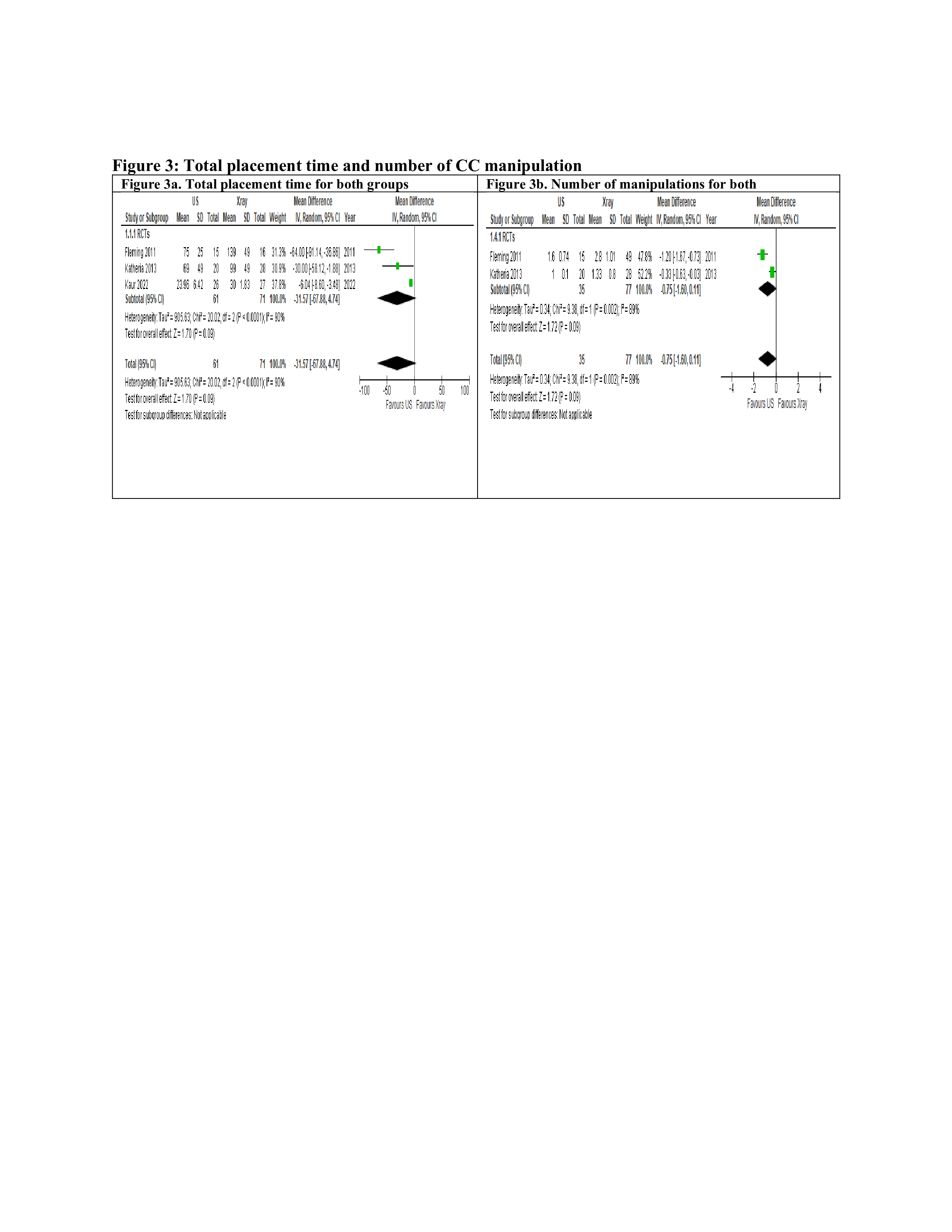
Background: Several small-scale randomized controlled trials (RCTs) and observational studies have undertaken comparisons between ultrasound-guided and radiography-guided central catheter (CC) placement in neonates. Objective: To systematically review and meta-analyze the available studies that compared ultrasound versus X-ray for the reduction of CC-associated complications in neonates. Design/Methods: We conducted searches of databases, including MEDLINE, COCHRANE, EMBASE, CINAHL, and clinicaltrials.gov, to identify RCTs and observational studies that evaluated ultrasound-guided versus X-ray-guided CC placement in neonates up to July 2023. To be eligible for inclusion, studies had to report one or more of the following outcomes: incidence of CC tip malposition, number of X-rays taken, total placement time, the number of CC manipulations required, and CC associated complications including central line associated bloodstream infection (CLABSI). We performed a meta-analysis using random effects models, utilizing aggregated data from all eligible studies. Forest plots were utilized to compare predefined outcomes across the included studies. The analysis was conducted using statistical software "Review Manager 5.4.1 and R 4.1.0." Results: Six studies, 4 randomized and 2 observational, involving 733 neonates were included in the analysis, with low risk of bias observed across all six studies. Ultrasound-guided CC placement was associated with significantly lower rates of CC malposition (5 studies, 703 participants, RR 0.45; 95% CI: 0.29-0.70). Similarly, ultrasound-guided CC placement was associated with significantly reduced number of X-rays required (3 studies, 386 participants, MD -0.89; 95% CI -1.6 to -0.2). However, there were no statistically significant differences in total procedure time (3 studies, 132 participants, MD -32 minutes; 95% CI -68 to 5 minutes), CC manipulations (2 studies, 112 participants, MD -0.75; 95% CI -1.6 to 0.11), and the incidence of CLABSI (2 studies, 328 participants, RR 1.35; 95% CI: 0.48-3.8). Other CC related complications such as extravasation, catheter occlusion, arrhythmia and cardiac tamponade were randomly reported in limited numbers to conduct a comprehensive analysis. All outcomes were evaluated as having low certainty of evidence based on the GRADE framework.
Conclusion(s): Based on low-grade of evidence, our analysis indicates that ultrasound-guided central catheter (CC) placement is associated with a reduction in the incidence of CC malposition and radiological exposure.
Registration: The protocol was registered in OSF (https://doi.org/10.17605/OSF.IO/HA9Q6)

 photo")
.jpg)