542 - Sex Differences in Health Service Utilization, Early Childhood Morbidity and Prescribed Medications by the Age of Five Among Children Born Preterm
Research Coordinator University of British Columbia University of British Columbia Vancouver, British Columbia, Canada
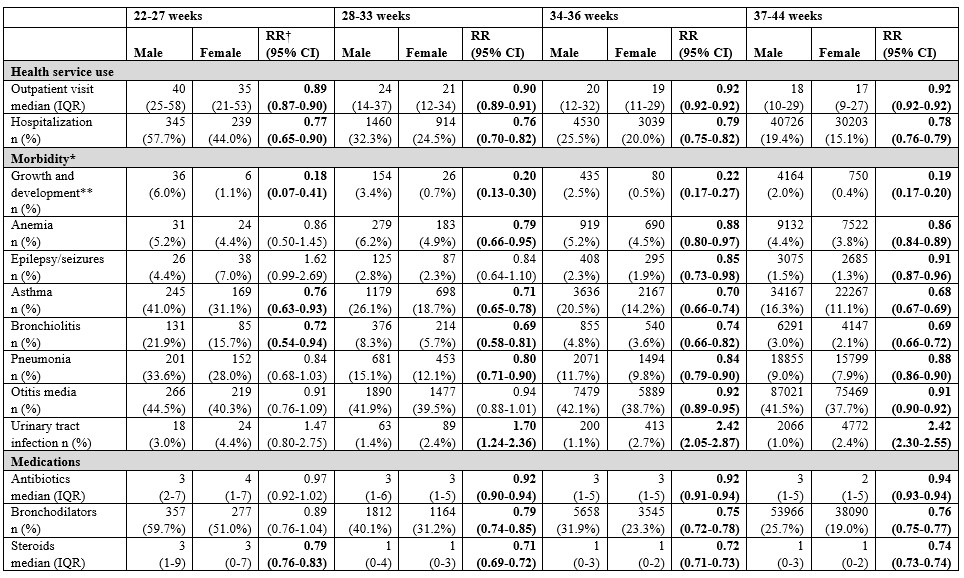
Background: Following preterm birth, male sex is an important risk factor for adverse neonatal outcomes and postnatal complications. There are limited population-based studies examining sex-specific health outcomes beyond the neonatal period among children born preterm. Objective: To determine whether health service use, morbidity, and medication use for up to five years of age differ between male and female children born preterm. Design/Methods: The study included liveborn infants at 22-44 weeks’ gestational age (GA) in British Columbia (BC), Canada, 2004-2014. Follow-up data to December 2019 included linked health information from four provincial databases (perinatal database, outpatient visits, hospitalizations, and outpatient prescriptions). The variable of sex was determined based on biological sex at birth. To compare sex-specific outcomes, incidence and rate ratios (RR) for health service use, childhood morbidity and medication use were analyzed within GA categories (22-27, 28-33, 34-36, 37-44) using Poisson regression. Results: This study included 455,960 children, with 51.4% being male and 48.6% female. Among them, 42,820 were born at less than 37 weeks’ GA, resulting in a preterm birth rate of 9.4%. The study findings are summarized in Table 1. Male children, regardless of GA category, had significantly more outpatient visits and more hospitalizations than their female counterparts by the age of five. Among children born at 34-36 weeks, females had significantly lower rates of growth and development problems (RR: 0.22, 95% CI: 0.17-0.27), asthma (RR: 0.70, 95% CI: 0.66-0.74) and bronchiolitis (RR: 0.74, 95% CI: 0.66-0.82), but higher rates of urinary tract infections (RR: 2.42, 95% CI: 2.05-2.87) compared to males. Rates of childhood morbidity increased with decreasing gestational age for both sexes. Females born at late preterm were prescribed fewer steroids (RR: 0.72, 95% CI: 0.71-0.73), bronchodilators (RR: 0.75, 95% CI: 0.72-0.78) and antibiotics (RR: 0.92, 95% CI: 0.91-0.94) than their male counterparts.
Conclusion(s): Compared to females, male children born preterm had higher rates of early childhood morbidity and had more outpatient visits, hospitalizations, and outpatient prescriptions by the age of five. These findings underscore the importance of considering biological sex in the context of health and development among children born preterm for clinical care and future research.

 photo")