College of Medicine University of Saskatchewan Saskatoon, Saskatchewan, Canada
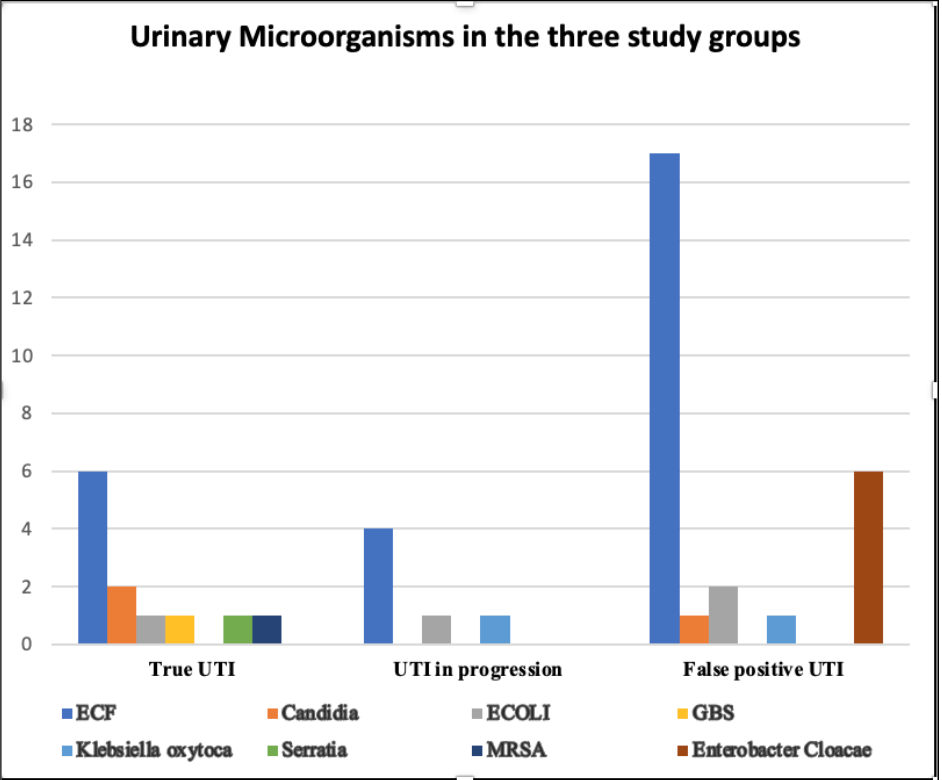
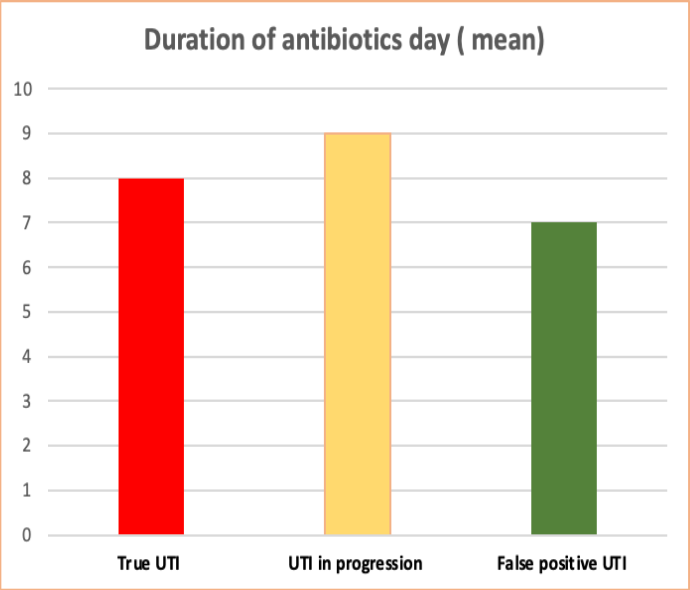
Background: Given that 30% of late onset sepsis in preterm infants is due to Urinary Tract Infection (UTI), UTI’s need to be routinely ruled out during septic workup in the Neonatal Intensive Care Unit (NICU). The reported prevalence of UTI is up to 13%. There is a noticeable paucity of guidance in the management at this age, with guidelines addressing those > 2 months. This lack of guidance leads to misdiagnosis and inappropriate antimicrobial use. Objective: We aimed to analyze our clinical practice surrounding the management of UTI in our NICU with infants born at < 32 weeks gestational age (GA). This study is part of a larger quality improvement study. Design/Methods: The chart review was conducted on preterm infants born at < 32 weeks (GA) in our level III NICU between January 2020 and December 2022. Three distinct UTI diagnostic criteria were created for accurate diagnosis of true UTI, UTI in progression, and false positive UTI with guidance from Canadian Paediatric Society and American Academy of Paediatrics guidelines on management of UTI. Results: Through ICD coding, a total of 43 episodes of UTI in 31 patients (prevalence 11%) were identified. As per the diagnostic criteria, 27 episodes were falsely positive with an alternate diagnosis. Enterococcus Faecalis was the most common organism identified. A total of 550 doses of the antibiotics were used in infants with falsely diagnosed UTI. We estimated that 218 doses of antibiotics could be avoided with false positive UTI diagnosis.
Conclusion(s): The three UTI diagnostic criteria developed can be used for correct diagnosis of UTI in preterm infants for judicious antimicrobial use. The UTI diagnosis criteria will be integrated in the clinical practice guideline for management of UTI in preterm infants.