Neonatal Fellow Neonatology Overland Park, Kansas, United States
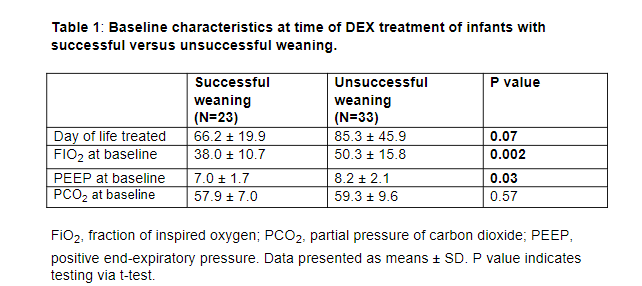
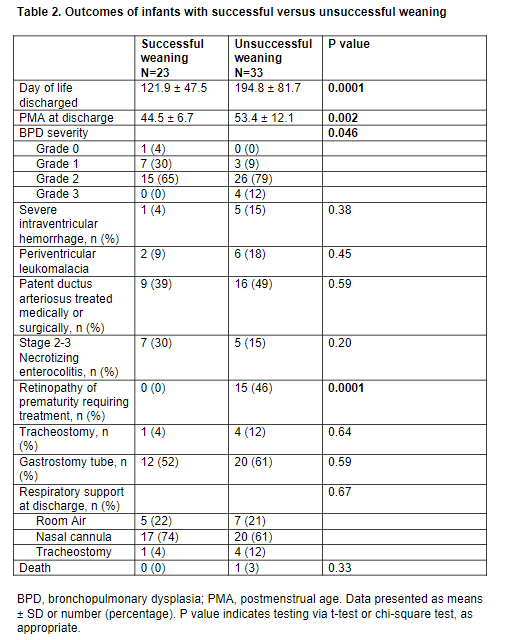
Background: Postnatal dexamethasone (DEX) has traditionally been reserved for preterm infants on prolonged mechanical ventilation, with reported rates of successful extubation at 47% to 76%. Recent emphasis on avoiding mechanical ventilation has resulted in preterm infants being increasingly supported with chronic non-invasive ventilation (NIV). The use of DEX for weaning preterm infants on chronic NIV remains largely unexplored. Objective: : To determine efficacy of postnatal DEX in weaning infants on chronic NIV, and to identify factors and outcomes associated with successful weaning. Design/Methods: Single-center retrospective study (2010-2022) of preterm infants ≤32 weeks' gestation treated with postnatal DEX while on chronic NIV. Data on baseline demographics, respiratory characteristics at start and end of treatment, and clinical outcomes were collected. Primary outcome was rate of successful weaning from NIV to high-flow nasal cannula (HFNC). Other outcomes included factors and outcomes associated with successful weaning. Results: A total of 56 infants (mean gestational age 26 weeks, mean birth weight 890 grams) received postnatal DEX while on NIV. The average postnatal day and postmenstrual age at time of treatment were 78 days and 37 weeks, respectively. DEX treatment resulted in a significant decrease in oxygen and ventilation support from baseline to end of treatment (Fig 1). Overall, the rate of successful weaning to HFNC was 46% (26/56). Infants treated with postnatal DEX for the first time had similar rates of successful weaning compared to infants who had received prior DEX treatment (43% vs 39%, P =0.79). Factors associated with successful weaning to HFNC were earlier age and lower NIV and oxygen support at time of DEX treatment (Table 1). Infants with successful weaning were more likely to be discharged earlier with less bronchopulmonary dysplasia and less retinopathy of prematurity compared to infants with unsuccessful weaning (Table 2). Other complications of prematurity were similar between the two groups (Table 2).
Conclusion(s): In our level IV NICU, efficacy of postnatal DEX to wean infants on chronic NIV was 46%. Our results suggest that DEX may also be useful in infants on chronic NIV, but further studies are needed to fully determine efficacy and safety.

.png)