41 - Feeding Problems in Neonates with Hypoxic Ischemic Encephalopathy Treated with Therapeutic Hypothermia and Association with Brain MRI and EEG Abnormalities
Associate professor Cleveland Clinic Children's Hospital Cleveland Clinic Children's Hospital Cleveland, Ohio, United States
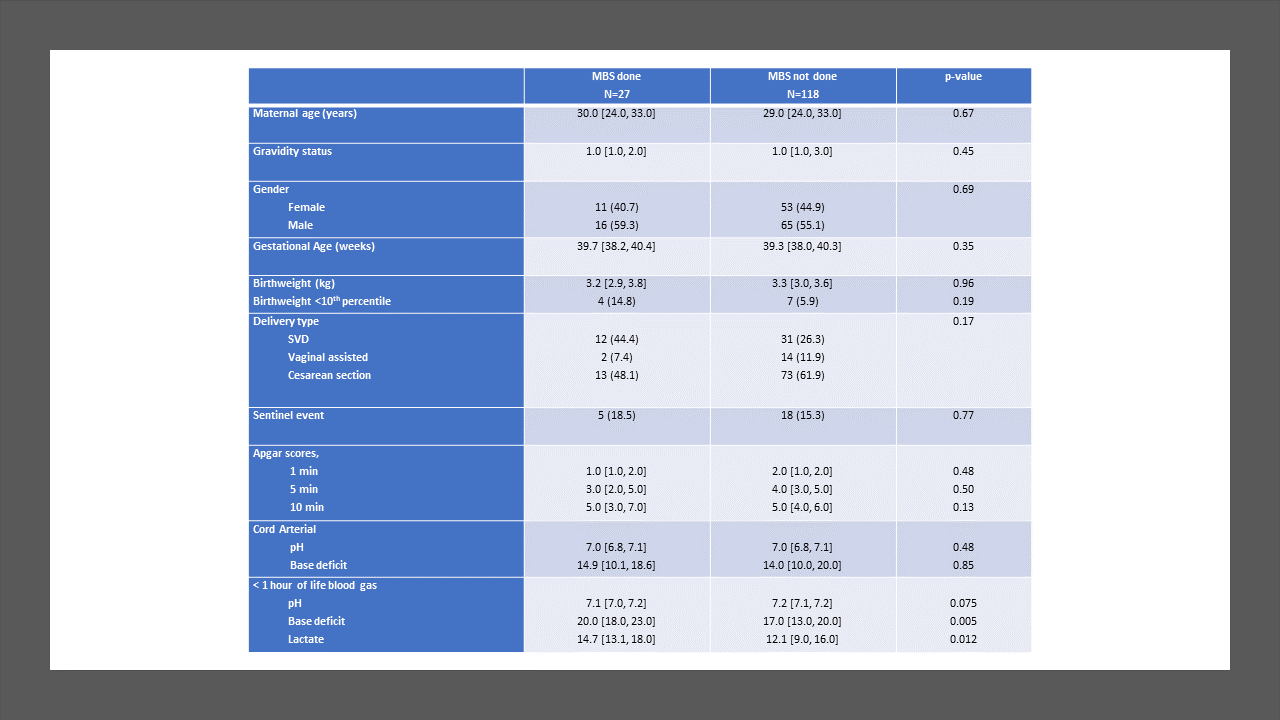
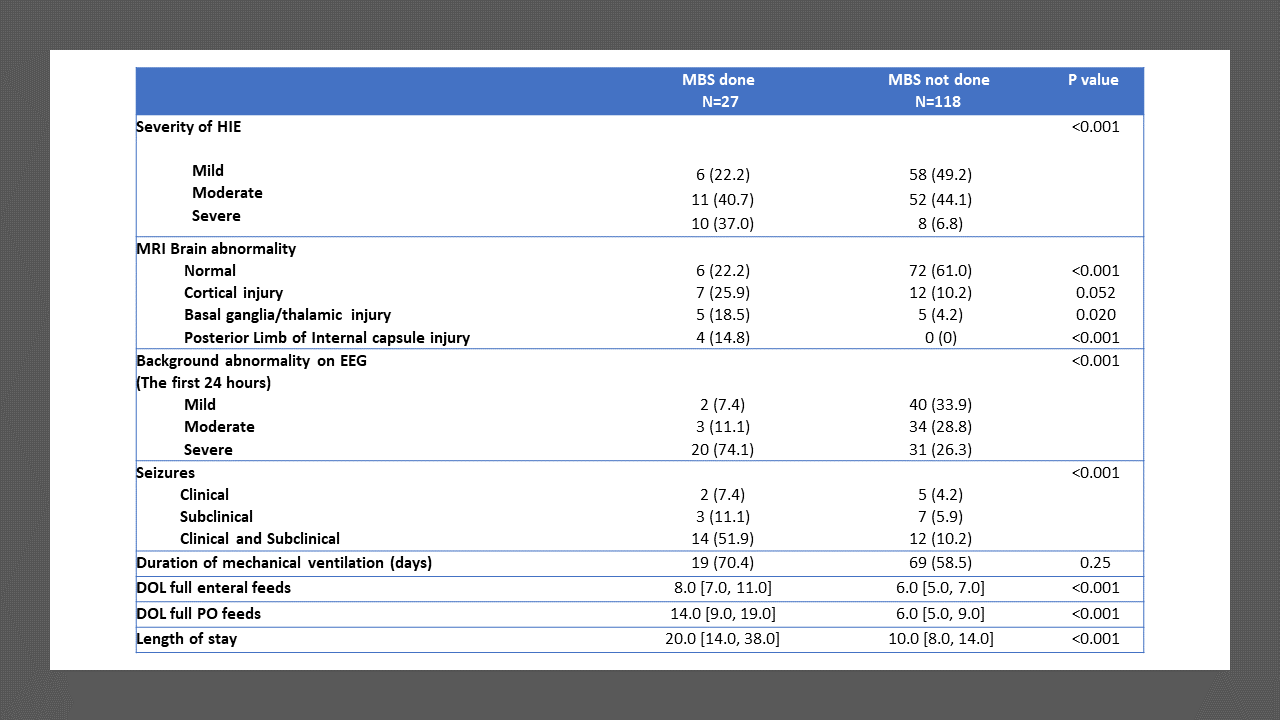
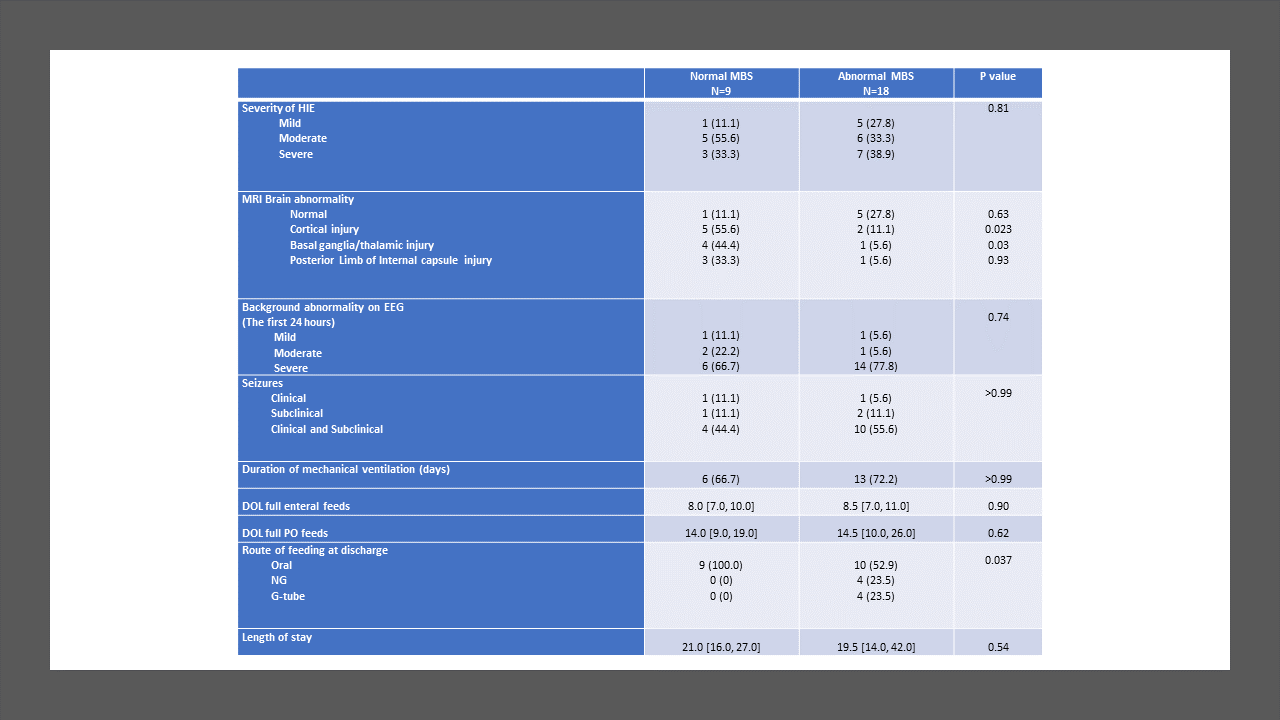
Background: Hypoxic Ischemic encephalopathy (HIE) is a major cause of morbidity and mortality in neonates. Early brain injury is known to have a deleterious impact on oral motor functions, which may lead to feeding and speech problems. Objective: To evaluate the prevalence of swallowing impairment and its association with brain magnetic resonance imaging (MRI) and electroencephalogram (EEG) abnormalities in neonates with HIE and treated with therapeutic hypothermia (TH). Design/Methods: This was a retrospective, single-center cohort study of HIE neonates (gestational age ≥ 36 weeks) who underwent TH between January 2012 and December 2022. Neonates with other significant congenital anomalies, genetic conditions, need for extracorporeal membrane oxygenation, or in-hospital mortality were excluded. Following rewarming, a modified barium swallow (MBS) was performed on neonates considered at risk for aspiration to identify swallowing impairment; brain MRI was performed in clinically stable babies (usually between 5-7 days of life). EEG was continuously performed from TH initiation till at least 80 hours of life. Results: In total, 145 neonates were included, with 55.9% males, 59.3% born by cesarean section, and 43.4/12.4% moderate/severe HIE. Median gestational age was 39.3 weeks. Overall, 27/145 (18.6%) MBS evaluations were performed: 9 (33.3%) normal, 8 (29.6%) dysphagia without aspiration, and 10 (37.0%) dysphagia with aspiration. Prevalence of abnormal swallow study was 7/18 (39%) in severe HIE, 6/63 (9%) in moderate HIE and 5/64 (8%) in mild HIE. Infants who required MBS had a significantly higher incidence of seizures, abnormal MRI, EEG, and longer hospital stay. Infants with abnormal MBS had more cortical, basal/thalamic ganglia injury compared to neonates with normal MBS. Among the infants who had abnormal MBS, only 8/18 (44 %) were discharged home on tube feeds: 4 with nasogastric and 4 with gastrostomy tube.
Conclusion(s): In this cohort of babies with HIE treated with TH, the prevalence of dysphagia was lower (overall 12.4%) than previously reported. Dysphagia improved in most babies by the time of discharge. Infants who required MBS had a significantly higher incidence of abnormalities on MRI. MBS should be limited to the babies with moderate to severe HIE.