380 - What is going on at the time of diagnosis? A prospective descriptive analysis of the activities and interactions that are competing for an emergency department doctor’s attention.
Medical Student Medical College of Wisconsin Wauwatosa, Wisconsin, United States
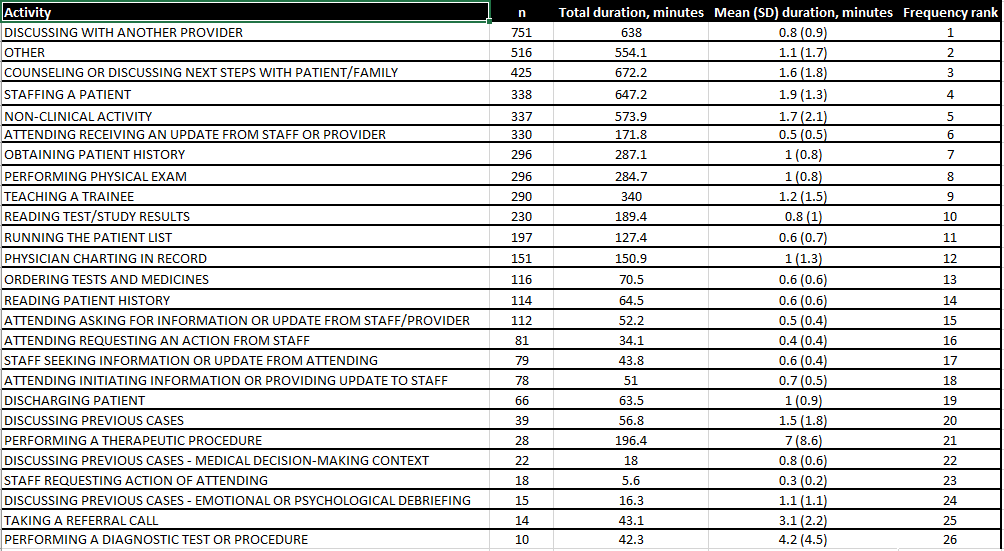
Background: Diagnostic error (DE) is the failure to accurately identify the etiology of a patient’s symptoms in a timely manner, and is a leading source of preventable harm, physician malpractice claims, and in-hospital mortality and morbidity. While DE has been the focus of patient safety work for over 15 years, there has been little progress in understanding or mitigation. Objective: This study utilizes naturalistic observation where observers recorded the tasks, tools, people, and environmental factors ongoing during the first hour of diagnostic work to provide information on the sociotechnical system that influences diagnostic decision making. Design/Methods: Guided by SEIPS 2.0 (System Engineering Initiative for Patient Safety) we created and tested a novel data collection tool in RECap. Observational data was collected on the tasks and interactions with people, tools, technologies, and environment during an attending physician’s diagnostic process in the pediatric emergency department. Results: This study was conducted July – August 2023 and included 21 unique attending physicians. Observers captured the first hour of 125 diagnostic encounters in 160 hours of observations, across 40 shifts. The average number of activities the physician conducted in this first hour was 48 (SD = 17). 40% of the activities utilized technology. The proportion of time spent in the patient room vs. workstation vs. unknown areas was 31%, 66% and 2%, respectively. The mean time spent in the patient room was 13.6 minutes versus time spent doing work for that patient outside the room was 28.6 minutes. The activities of the attending physician are summarized in table 1.
Conclusion(s): While the DE literature has described a multidisciplinary team in performing a diagnosis, the nature and amount of communication has not been described. We observed that 40% of the tasks rely on tools and technologies. The physician spends more time caring for the patient outside the patient’s room than in the room. To date, there is no such characterization of physician diagnostic work in context. These results demonstrate that the diagnostic process includes many complex interactions with people, tools, and their environment. Further, the physician does not have protected time for each patient, but instead performs many competing tasks and interactions requiring task switching and divided attention. Understanding the context of the diagnostic process is paramount to understanding and minimizing diagnostic error.

 photo")