Assistant Professor The University of Western Ontario - Schulich School of Medicine & Dentistry London, Ontario, Canada
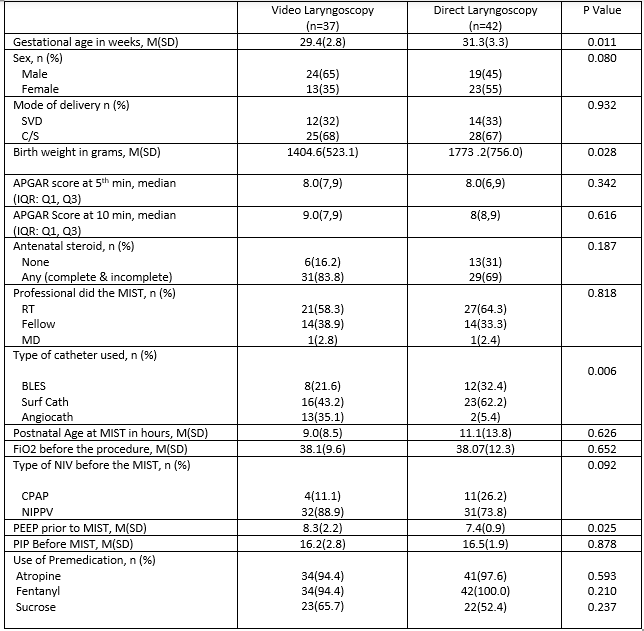
Background: Minimally invasive surfactant therapy (MIST) has emerged as a preferred method of surfactant administration. Pioneers of this technique have described the use of direct laryngoscopy (DL) for MIST. With the increasing application of video laryngoscopy (VL) for neonatal airway management, it is speculated that MIST techniques can be adapted to use with VL. Objective: To compare procedural success, operator ease of use, and complication of MIST using VL vs. MIST using DL. Design/Methods: A retrospective, observational cohort study was conducted at a tertiary-level neonatal intensive care unit after obtaining ethical approval. Neonates receiving MIST between October 1, 2020, and October 31, 2022, were included. Baseline demographic characteristics and procedural data were collected. The primary outcome included the overall procedural success rate, the need for multiple attempts, and the total number of attempts. Means (SD), independent t-tests, frequencies (%), and chi-square were used as appropriate. P-values < 0.05 were considered statistically significant. Results: Of 79 neonates included, 37 neonates received MIST via VL and 42 received MIST via DL. (Table 1). Mean gestational age (GA) was lower in VL group compared to DL group, [29.2 weeks vs 31.3 weeks respectively; p=0.011]. Mean (SD) birthweight (BW) in VL group was lower than DL group [1404.6 g (523.1) vs 1773.2 (756.0), respectively; p=0.028]. Purpose built catheter use was lower in VL vs DL [24(64.8%) vs 35(94.5%) respectively; p=0.006]. Positive-end expiratory pressure (PEEP) prior to MIST was higher in VL vs DL [8.3(2.20 vs 7.4(0.9), p=.025]. Overall procedural success was similar between groups (Table 2). The need for multiple attempts was lower with VL in comparison to DL [n=4 (11%) vs n=13 (31%), respectively; p= 0.034)] at bivariate level, but was not significant in a multivariable model correcting for GA, BW, PEEP level, and catheter type. (p=0.131). Procedural complications, the need for second dose of surfactant, the need for mechanical ventilation post-MIST, and operator ease of use were similar between MIST groups. User comments emphasized the value of VL in providing real-time visual information to confirm catheter placement and guide operators/trainees.
Conclusion(s): Procedural success, complications, and operator ease of use for MIST using VL and DL were comparable despite VL being a more recently adapted technology, and being used more in smaller, sicker, and more premature neonates. Our findings show successful application of VL for MIST and suggest a procedural advantage that might facilitate universal adoption.

 photo")
.png)