Fellow, PGY-5 Children's Hospital of Richmond at VCU Henrico, Virginia, United States
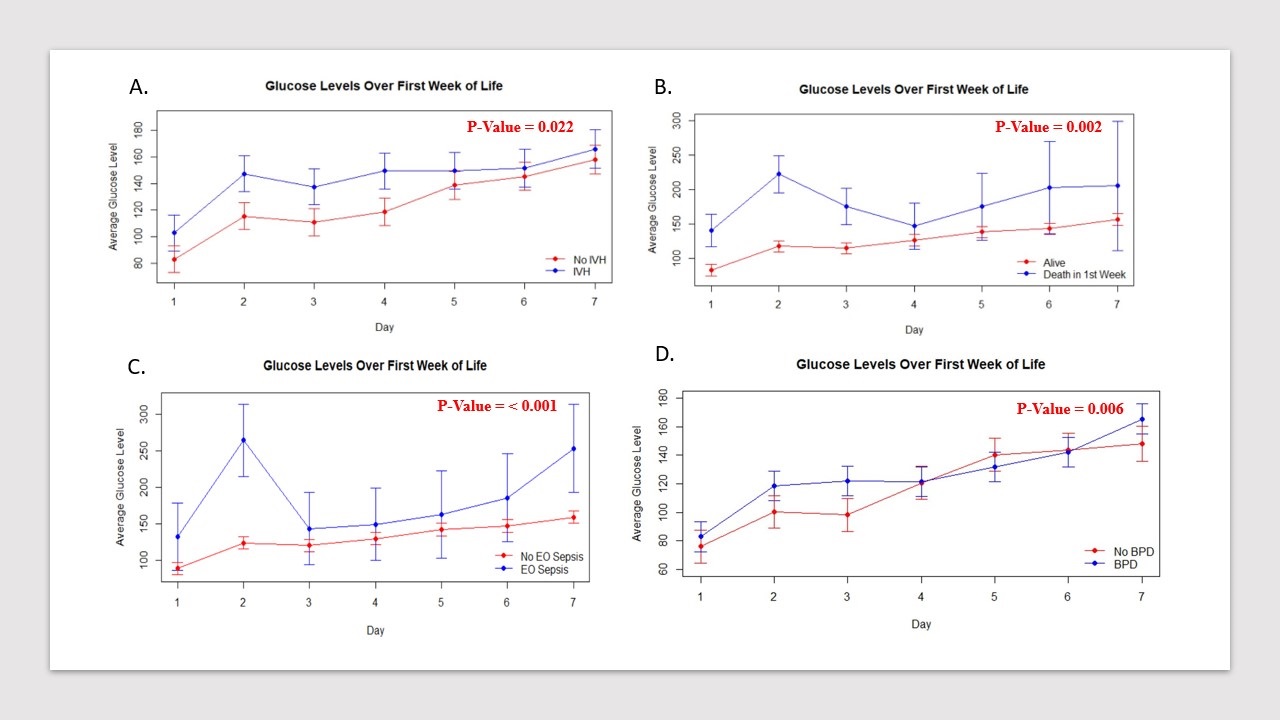
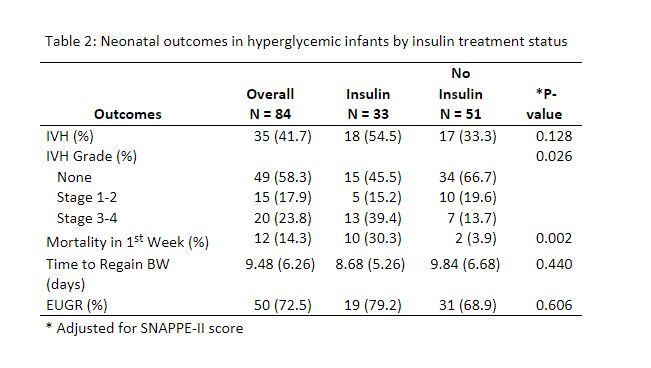
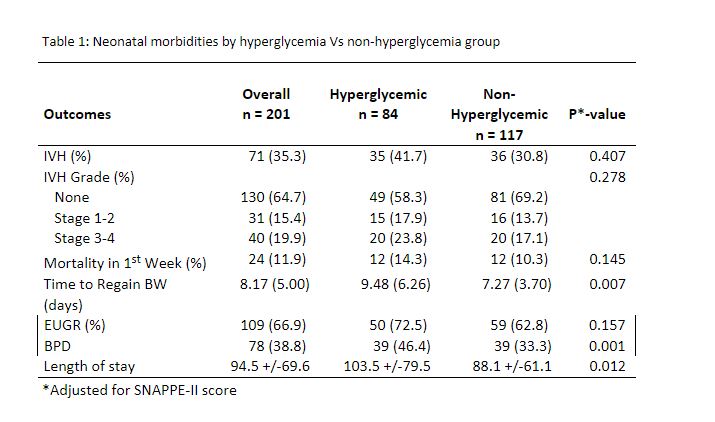
Background: Hyperglycemia in ELBW infants (ELBW) is common and poorly defined. Studies have shown osmotic changes with glucose levels ≥180 mg/dl could be associated with an increased risk of intraventricular hemorrhage (IVH) and mortality. Management of hyperglycemia in ELBW consists of a lower glucose infusion rate and use of exogenous insulin. These can lead to poor caloric delivery, catabolism, and hypoglycemia. We hypothesize that ELBW infants with hyperglycemia (2 blood glucose levels of ≥180 mg/dL over a 4hr span) in the first week of life have a higher risk for IVH, and mortality with no benefit on time to regain birth weight (BW). We also hypothesize that insulin treatment does not impact short-term morbidities related to hyperglycemia. Objective: Determine the effect of: 1. Hyperglycemia and risk of IVH, mortality, time to regain BW, and extrauterine growth restriction (EUGR) in the first week of life. 2. Insulin treatment on the association of hyperglycemia and morbidities. Design/Methods: Retrospective chart review of all ELBW admitted to our level IV NICU within the first 12 hours of life from January 2017-December 2022. Glucose levels within the first 7 days of life, maternal and infant characteristics were documented. We analyzed the association of first week of life glucose trends with morbidities. Severity of illness was adjusted using SNAPPEII score. Descriptive analysis, T-tests, Chi-Square, and RMANOVA were used for statistical analysis. Results: A total of 224 ELBW were analyzed with 23/224 excluded. Average gestational age was 25.7 +/- 2.2 weeks with a BW of 726.2 +/- 174.4g, and 84/201 qualified as having hyperglycemia. No significant difference was noted for risk of IVH, mortality and EUGR between hyperglycemic and non-hyperglycemic groups after adjusting for severity of illness. Those with hyperglycemia had increased risk for bronchopulmonary dysplasia (BPD), prolonged hospital stay, and time to regain BW (Table1). IVH, first week mortality, BPD, and early onset sepsis was seen with higher daily average glucose levels (Figure1. a-d). Insulin treatment (33/84) showed greater risk for IVH and first week mortality (Table2).
Conclusion(s): Hyperglycemia in ELBW was associated with a higher risk for BPD, prolonged hospital stay, and prolonged time to BW. Higher daily average glucose values increased the risk of IVH, early onset sepsis, BPD, and early death. Insulin treatment was not associated with any short or long-term optimal growth outcomes but was significantly associated with greater risk of IVH, and mortality in the first week of life.