4 - Changes in Treatment and Outcomes in Late Preterm and Term Infants with Hypoxic Ischemic Encephalopathy Over Time in a Large California Neonatal Cohort
Neonatology Fellow University of California, San Diego School of Medicine San Diego, California, United States
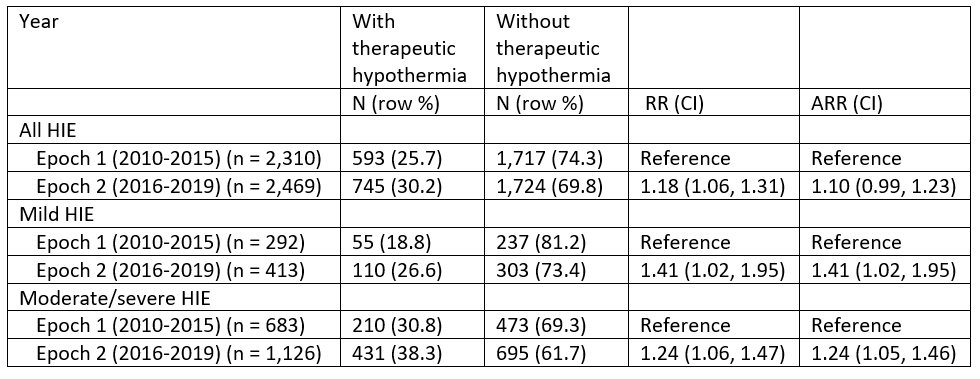
Background: Hypoxic ischemic encephalopathy (HIE) is a leading cause of mortality and morbidity in term neonates. Therapeutic hypothermia (TH) has been the standard treatment for HIE for fifteen years. Following landmark studies in 2015, TH has been applied to a wider range of infants including those with mild HIE despite limited evidence of benefit. Objective: The objective of this study was to evaluate the change in management of infants with different severities of HIE and outcomes over time. Design/Methods: We queried an administrative birth cohort in California from 2010-2019 using ICD codes and divided those infants into two epochs, Epoch 1 (2010-2015) and Epoch 2 (2016-2019) to evaluate how the application of TH and adverse outcomes of infants with HIE has changed over time. Log-linear regression was used to calculate risk ratios (RR) for TH in each epoch for all HIE, mild, and moderate/severe HIE. Risk of adverse infant outcome was calculated for each severity of HIE. Results: In the sample cohort, 4779 infants with HIE were identified. For any HIE, 593 (25.7%) infants received TH in Epoch 1, and 745 (30.2%) infants in Epoch 2 received TH. The unadjusted risk ratio (RR) for TH for Epochs 2 compared to Epoch 1 for infants with any HIE was 1.18 (CI 1.06 to 1.31), which attenuated upon adjustment (aRR 1.10; CI 0.99 to 1.23). There was a significant increase in TH for infants diagnosed with mild HIE in Epoch 2 compared to Epoch 1 (26.6% Epoch 2 vs 18.8% Epoch 1, aRR 1.41 (95% CI 1.02-1.95). For infants with any HIE that did not receive TH there was a decreased risk of any adverse event (aRR 0.9; CI 0.8 - 0.97), gastrostomy placement (ARR 0.5; 95% CI 0.4 -0.7), and tracheostomy placement (aRR 0.5; 95% CI 0.2 - 0.9) in Epoch 2 compared to Epoch 1. Infants in Epoch 2 had decreased mortality compared to Epoch 1, whether they received TH (ARR 0.5; 95% CI 0.3- 0.8) or not (aRR 0.7; 95% CI 0.5-0.9) . There were no significant differences between epochs for infants with mild HIE and received TH. There was no significant difference in cerebral palsy between epochs for any severity of HIE.
Conclusion(s): Significantly more infants with mild HIE received TH since 2015, but this study found no difference in outcomes over time for these patients. For infants with any HIE there was improvement in mortality, which likely represents progress in technology and management over time. This study was limited by the use of ICD 9/10 codes and a one year follow up time. Clearer guidelines for the categorization of HIE severity may be beneficial for evaluating the increased use of TH in mild HIE.

 photo")