Senior Staff Specialist Neonatology Mater Mothers' Hospital South Brisbane, Queensland, Australia
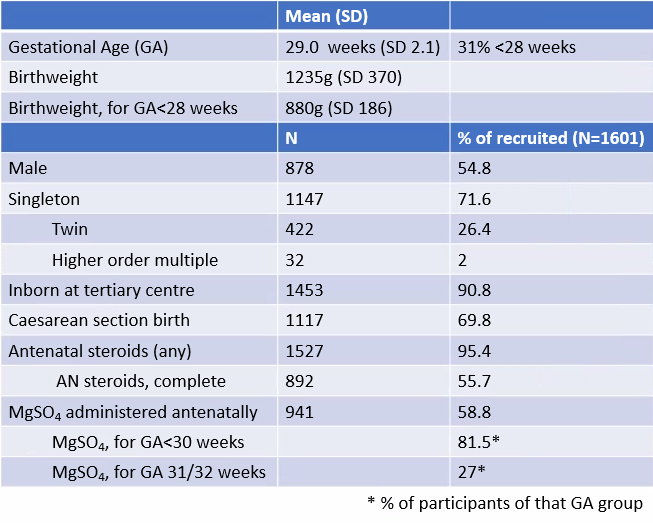
Background: Antenatal maternal magnesium sulfate (MgSO4) administration is a proven efficacious neuroprotective treatment reducing the risk of cerebral palsy (CP) among infants born preterm. This study’s novel hypothesis postulates that sulfate is the neuroprotective component; not previously considered, yet with strong scientific rationale. Objective: To determine whether there is a relationship between plasma SO4 and/or Mg concentration in Very/Extremely Preterm (VP/EP) infants at 7 days of age (d7) and adverse neurodevelopmental outcome at 2 years corrected age (CA), with VP/EP subgroup analysis. Design/Methods: Prospective observational cohort study, recruiting preterm infants born 2013-2020 at gestational age (GA) 24+0 to 31+6 and followed up at 2 years CA. Data collected on MgSO4 exposure (dose/duration/timing). Blood sample d7 for plasma SO4/Mg measurement. Multiple blood samples in subset on days 0,3,7,14,28. Follow up assessments for CP, cognitive/language/motor development, and social/behavioral difficulties. Sample size: 1324 infants with follow-up data are required to determine 30% relative risk (RR) reduction in CP (from 7%) when plasma sulfate is 1 SD above mean (80% power, type I error 0.05). [Cochrane Review, MgSO4: 29% RR reduction] Recruitment target 1600 (~17% death/loss). Results: 1601 participants. Table 1 gives descriptive statistics; Table 2 – blood collection, survival, follow-up. Plasma sulfate concentration (PSC) falls rapidly in first 3 days. Antenatal MgSO4 is associated with supra-physiological PSC at birth. Physiological PSC at birth (no MgSO4), and the difference between d0 & d7 PSC, are GA dependent. With decreasing GA, PSC increases and d0-7 fall is greater. Using d7 PSC adjusted for GA, and AUC d0-7 for subset with multiple samples, the relationship between plasma SO4/Mg concentration & neurodevelopmental outcome will be presented.
Conclusion(s): This study has discovered previously unknown GA dependence of fetal PSC. GA-dependence of the magnitude of d0-7 fall in PSC suggests that EP infants may be more vulnerable (a priori EP subgroup analysis). If follow-up data (which will be presented) confirms an association of higher risk of disability when PSC is low-for-GA, but no relationship with plasma Mg, the study hypothesis of the neuroprotective role of sulfate is supported. Neonatal sulfate supplementation with target PSC could potentially reduce the risk of disability, with greater efficacy and accessibility than MgSO4. This would be a significant advancement in preterm care, benefiting preterm infants, families and society. Funded by NHMRC, Mater Foundation, CP Alliance

 photo")
.png)