Attending Neonatologist/Assistant Professor Cincinnati Children's Hospital Medical Center 45229, Ohio, United States
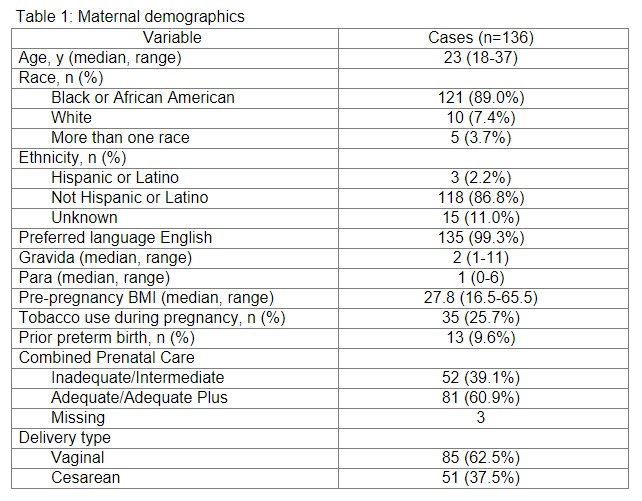
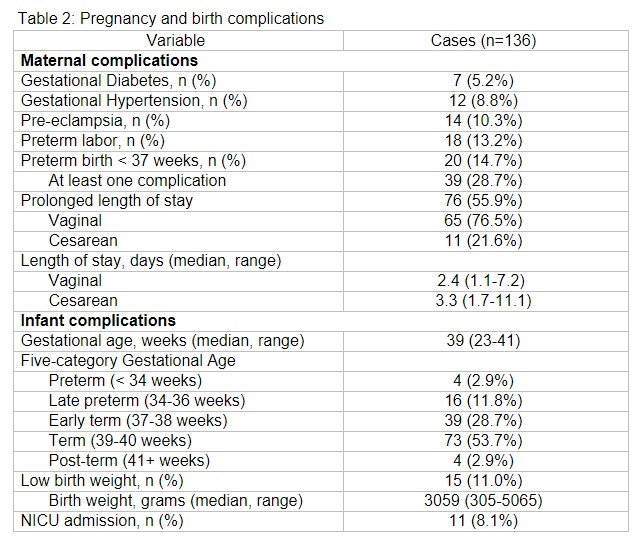
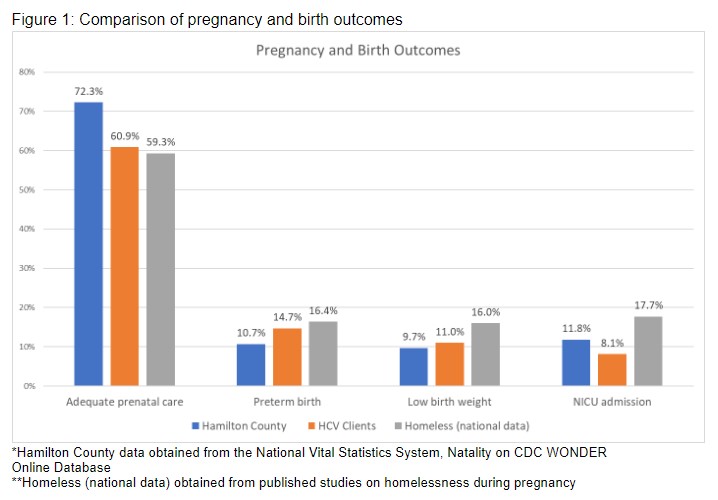
Background: Homelessness during pregnancy poses significant health risks for pregnant individuals and their infants. Limited data exists on the effect housing provision may have on pregnancy and birth outcomes. The federal Housing Choice Voucher (HCV) program helps qualifying clients pay for housing. Local public housing authorities may prioritize high-risk populations to bypass multi-year HCV waitlists. In 2018, the Cincinnati Metro Housing Authority prioritized pregnancy for HCV provision, a novel intervention. Objective: To characterize healthcare utilization patterns (adequacy of prenatal care, prolonged length of stay) and birth outcomes (preterm birth, low birthweight, neonatal intensive care [NICU] admission) in pregnant clients prioritized for HCV in Hamilton County, OH. Design/Methods: This observational retrospective review included 136 pregnant clients from 1/1/2018 to 12/31/2021. Descriptive statistics summarized the distribution of chosen outcomes and were compared to county-based birth outcomes and national birth data in the homeless population. Results: Clients were majority non-Hispanic Black and multigravid/multiparous (Table 1). Most (82.4%) had ≥ 1 pregnancy risk factor (pre-conception BMI < 18.5 or > 24.5, age < 20 or > 34 years, tobacco use, prior preterm birth). 61% received adequate prenatal care as defined by the Adequacy of Prenatal Care Utilization Index. Pregnancy complications (gestational hypertension, gestational diabetes, pre-eclampsia, preterm labor) are shown in Table 2 and affected 29% of clients. 19% of infants were born preterm, low birth weight, or required NICU admission. 56% experienced prolonged maternal length of stay using a standard obstetric definition based on delivery mode. Population-level pregnancy and birth complication rates in Hamilton County and in previously published studies of homeless pregnant individuals are shown in Figure 1 for comparison.
Conclusion(s): Pregnant individuals granted priority HCVs received adequate prenatal care at lower rates and experienced higher rates of preterm birth and low birth weight compared to local norms. Over half experienced prolonged maternal birth hospitalizations. Conversely, HCV clients had higher rates of adequate prenatal care and lower rates of preterm birth and low birthweight compared to published outcomes of homelessness in pregnancy.
Additional analysis using a propensity score model and regression to analyze outcomes compared to a cohort of pregnant Ohioans reporting homelessness or housing instability a year prior to birth who did not have access to housing prioritization is ongoing.

 photo")