Professor of Pediatrics Cincinnati Children's Hospital Medical Center Cincinnati, Ohio, United States
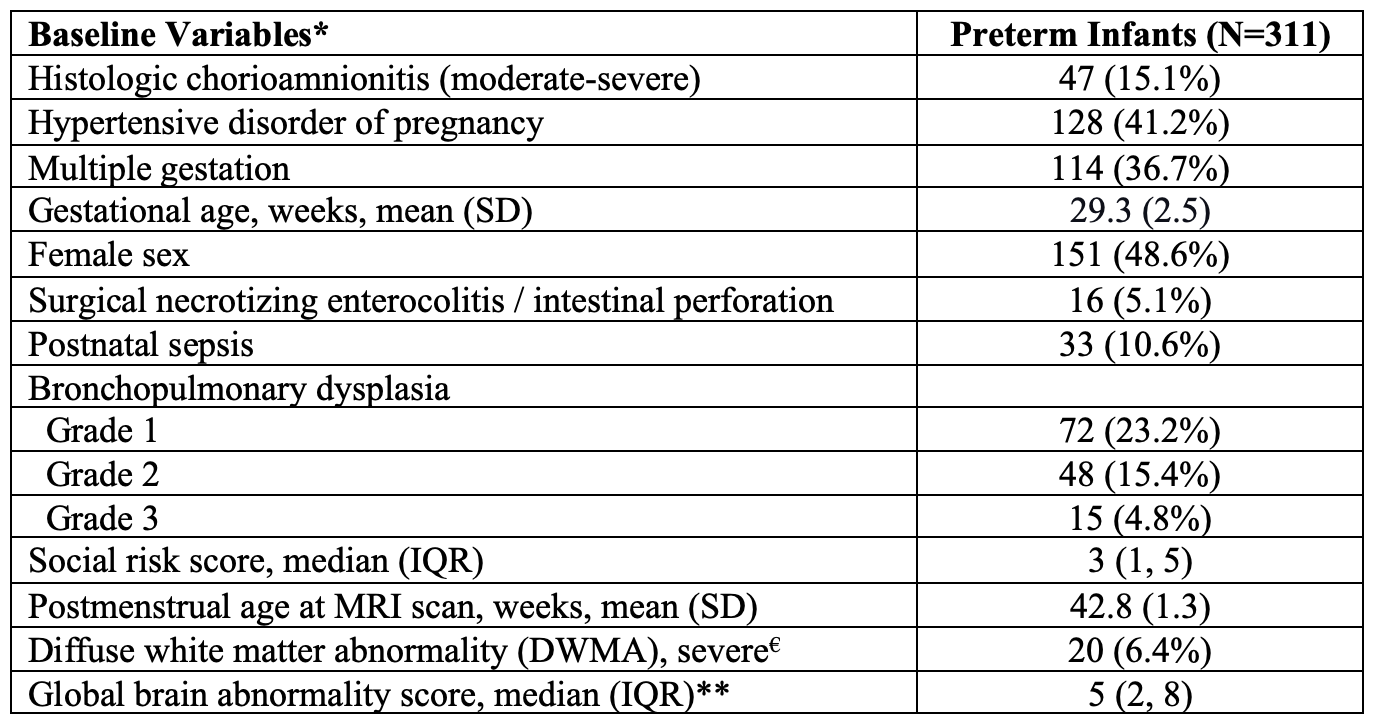
Background: Cognitive impairment remains the most common long-term adverse outcome following preterm birth. Accurate diagnosis takes 3 to 5 years during which time we are missing an early critical window of neuroplasticity. Detection during this window would enable early targeted interventions that can enhance therapeutic efficacy. Objective: To improve early prediction of cognitive development by exploiting features from brain diffusion MRI, resting state functional MRI, and structural MRI. Design/Methods: We assembled a multisite regional cohort of 358 preterm infants (≤32 weeks’ gestation) from 5 Southwest Ohio NICUs (CINEPS cohort). All infants were imaged at term-equivalent age on the same 3T Philips MRI scanner using harmonized MRI sequences. Cognitive development was assessed with the Differential Ability Scales (2nd Edition) General Conceptual Ability (GCA) score at 3 years corrected age. We used atlases from the Developing Human Connectome Project to derive ~20,000 brain features from structural connectivity (SC), functional connectivity (FC) and morphometry (brain volumes; cortical maturation measures). We used graph theory and non-negative matrix factorization (NMF) for unsupervised feature selection. Last, support vector machine (SVM) was applied to develop a multimodal model to predict individual GCA scores. We created 500 bootstrap datasets to evaluate model performance and correct for over-optimism per the Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD) guidelines. To assess model fit, we calculated optimism corrected values for R2, root mean square error (RMSE), and difference between observed and predicted scores. Results: The mean (SD) gestational age was 29.3 (2.5) and GCA score was 93.7 (20.1) for the 311 infants (87%) with follow-up data at or after 3 years CA (Table 1). Each advanced MRI modality achieved reasonable prediction accuracy individually, and the multimodal model combining all 3 MRI modalities offered the highest accuracy with an optimism corrected R2 value of 64.1% (95% CI: 55.5, 71.8). The predicted cognitive scores of the multimodal model were closely aligned with the observed scores (Fig. 1A); 68.8% of the predicted GCA scores were within +/- 6.5 points (1 SD) of the observed scores (Fig. 1B).
Conclusion(s): In a regional prospective cohort of preterm infants, we developed and internally validated a model for early, accurate prediction of long-term cognitive development. This model can be utilized for early detection and targeted enrollment of preterm infants for cognitive stimulation therapies.


.png)
.png)