Professor Baystate Children's Hospital Springfield, Massachusetts, United States
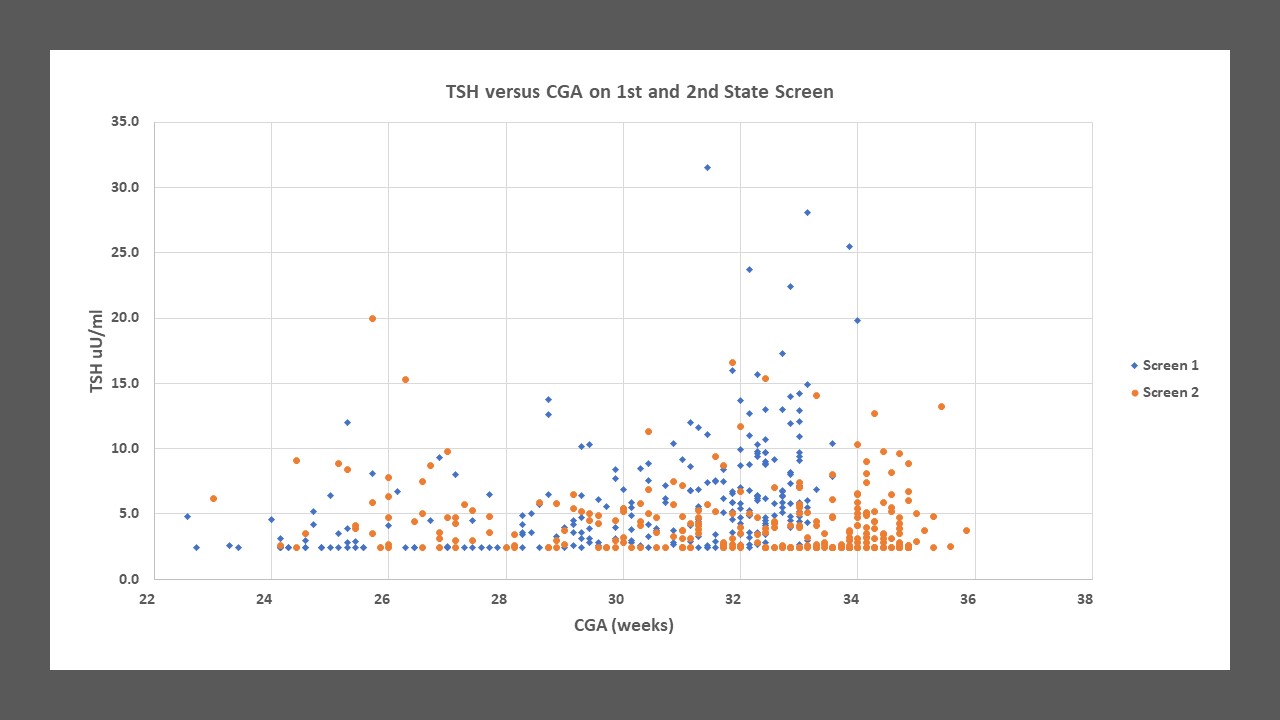
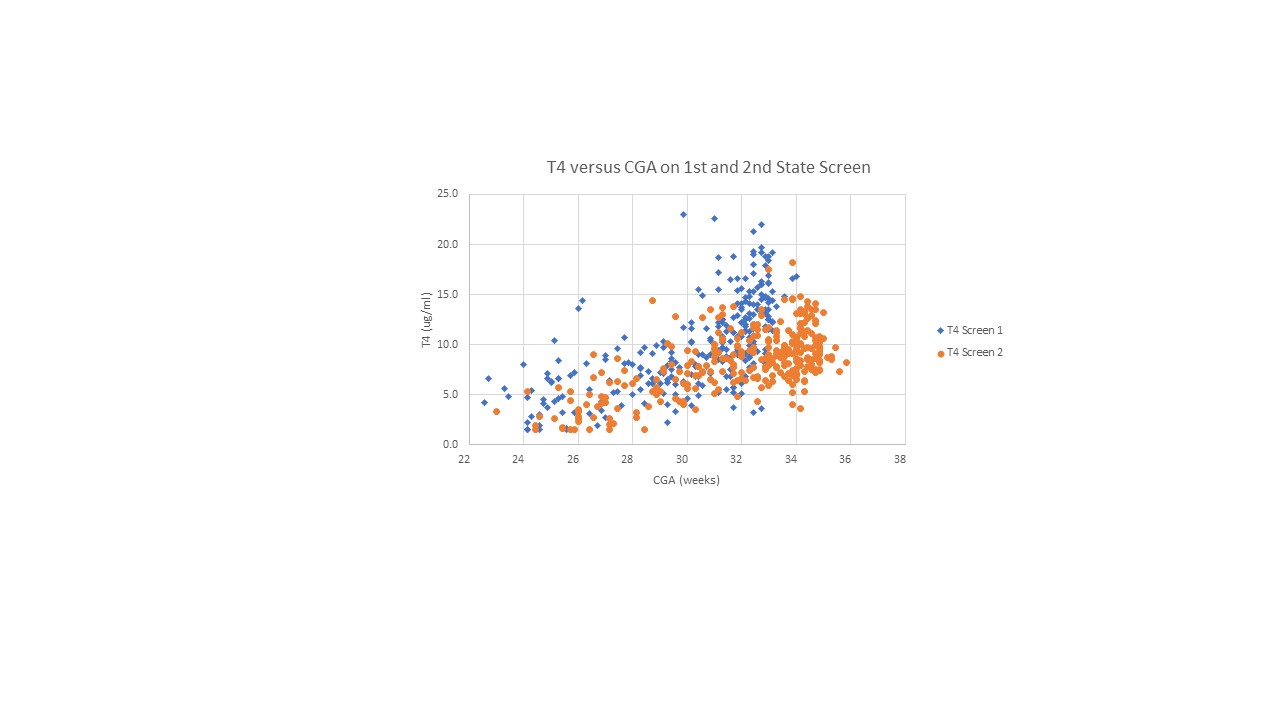
Background: Thyroid hormones are important for the development and maturation of lung and brain tissue. Levels of T4 and TSH vary with gestational age, postnatal age, and clinical condition of the infant. Sick and/or preterm infants may not be able to stimulate TSH production in the face of low T4. In order to identify congenital hypothyroidism, the mandated state screen has set normal TSH levels of < 15uU/ml or < 10 uU/ml for first and second screen, respectively. Objective: The purpose of this study is to evaluate if the “normal” levels of TSH on the first and second state screen are appropriate to identify infants born at < 34 weeks who are at risk for hypothyroidism. Design/Methods: All infants born at < 34 weeks gestation in 2021-2022 who had results of the mandated state screen were enrolled in this study. Clinical information was obtained from the infant’s EMR. TSH levels below the threshold of measurement ( < 2.5 uU/ml) were given a value of 2.4 and T4 levels < 1.6 ug/dl were given a value of 1.5. This study was granted a waiver of consent by the IRB as it is a retrospective study. Results: Newborn state screen results were available for 283 infants. TSH was at the lower limit of measurement in 21% and 33% of first and second screens, respectively. The first, second, and third quartile for TSH on the first state screen was 2.8/4.8/7.5 and 2.4/3.3/5.0 uU/ml on the second state screen. There was a linear relationship between T4 and CGA but no relationship between TSH and CGA or between TSH and T4. The relationship between corrected gestational age (CGA) and TSH and T4 for the first (day 0-5) and the second (day 6-20) state screen is shown in graph 1 and 2, respectively. Seven infants were treated with levothyroxine and data is depicted in Table. Two infants had markedly elevated TSH and low T4 on the second state screen and were treated within the first 3 weeks of life. Two infants developed hypothyroidism with low fT4 (0.41 and 0.2 ng/dL) 2-3 weeks after an unremarkable state screen and were treated at about 1 month of age. Two infants were treated for clinical hypothyroidism. One infant was treated with levothyroxine due to low serum fT4 with low TSH.
Conclusion(s): About 1/3 of infants had an TSH below detection limits during the first 3 weeks of life. In preterm infants, significant elevation in TSH may not occur despite a very low fT4 and subtle elevation in TSH may indicate hypothyroidism that should prompt evaluation of serum levels of fT4 an TSH. Relying on state screen cutoff of TSH may not Identify infants at risk for developing hypothyroidism who might benefit from treatment.

.jpg)