Assistant Professor UAB Birmingham, Alabama, United States
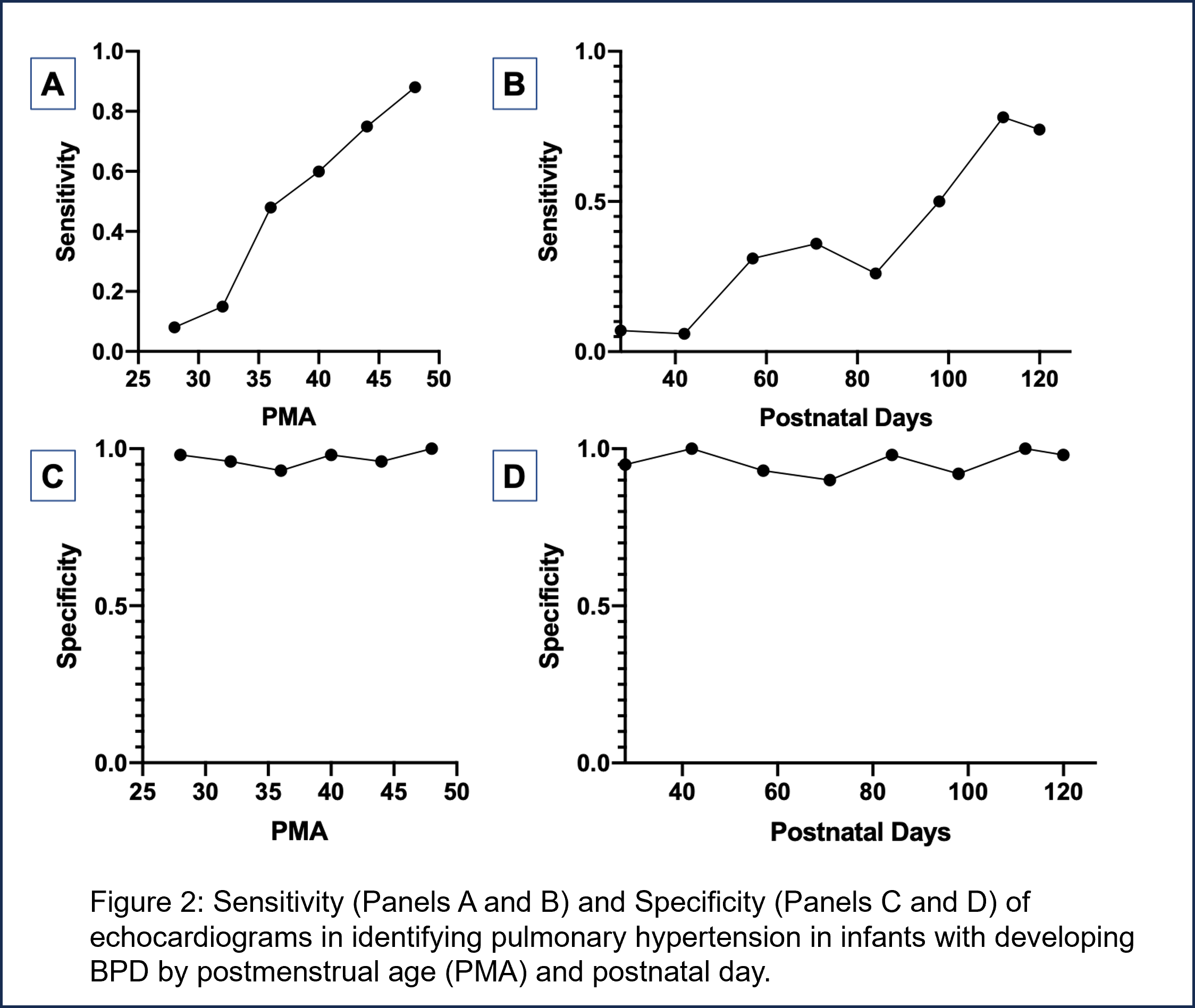
Background: Bronchopulmonary dysplasia associated pulmonary hypertension (BPD-PH) is the most severe endotype of BPD, however, there is insufficient evidence to suggest the optimal screening strategy in at risk infants. The recommendation by the American Heart Association is to screen infants with BPD for PH at 36 weeks’ postmenstrual age. Despite this important recommendation, the diagnostic accuracy of echocardiographic screening over the course of hospitalization has not been determined. Objective: We hypothesized that serial echocardiography throughout hospitalization would improve PH detection with an anticipated high negative predictive value with early screening and increasing positive predictive value with increasing postnatal age. Design/Methods: This was a prospective single center study conducted between 2017 and 2020. In infants with BPD-PH, all echocardiograms preceding a diagnostic echocardiogram were included and considered false negatives for prediction of later PH. Echocardiograms subsequent to diagnosis in infants with BPD-PH were used in assessing whether a diagnostic echocardiogram was a true positive (in the instance that PH was again demonstrated) or a false positive (in the instance that PH was no longer observed). In infants with BPD alone, all echocardiograms were included and were considered true negatives. These indices were then used to estimate the sensitivity, specificity, positive predictive value, and negative predictive value of echocardiographic screening for PH. BPD-PH related outcomes (e.g. mortality and PH resolution by discharge) were related by the time of diagnosis (either before or after 36 weeks’ postmenstrual age (PMA)). Results: Data from 220 infants were available for this analysis of whom 138 had BPD alone and 82 had BPD-PH. Nine hundred twenty-four echocardiograms were used in estimates of diagnostic accuracy. The highest negative and positive predictive values were demonstrated beyond 36 weeks’ postmenstrual age (Figure 1). Echocardiogram sensitivity remained low for the majority of hospitalization whereas specificity remained high throughout hospitalization (Figure 2). Infants with BPD-PH diagnosed before 36 weeks’ PMA were initiated on sildenafil at a lower PMA (34w vs 48w; p=0.0001) but did not have a lower rate of PH resolution (59% vs 42%; p=0.17) or mortality (24% vs 23%; p=1.00).
Conclusion(s): For earlier identification of infants with BPD-PH, echocardiographic PH screening had high sensitivity throughout hospitalization; however, serial echocardiography may be useful given the low testing sensitivity and high false negative rate.


.png)