Clinical Assistant Professor Stanford University Palo Alto, California, United States
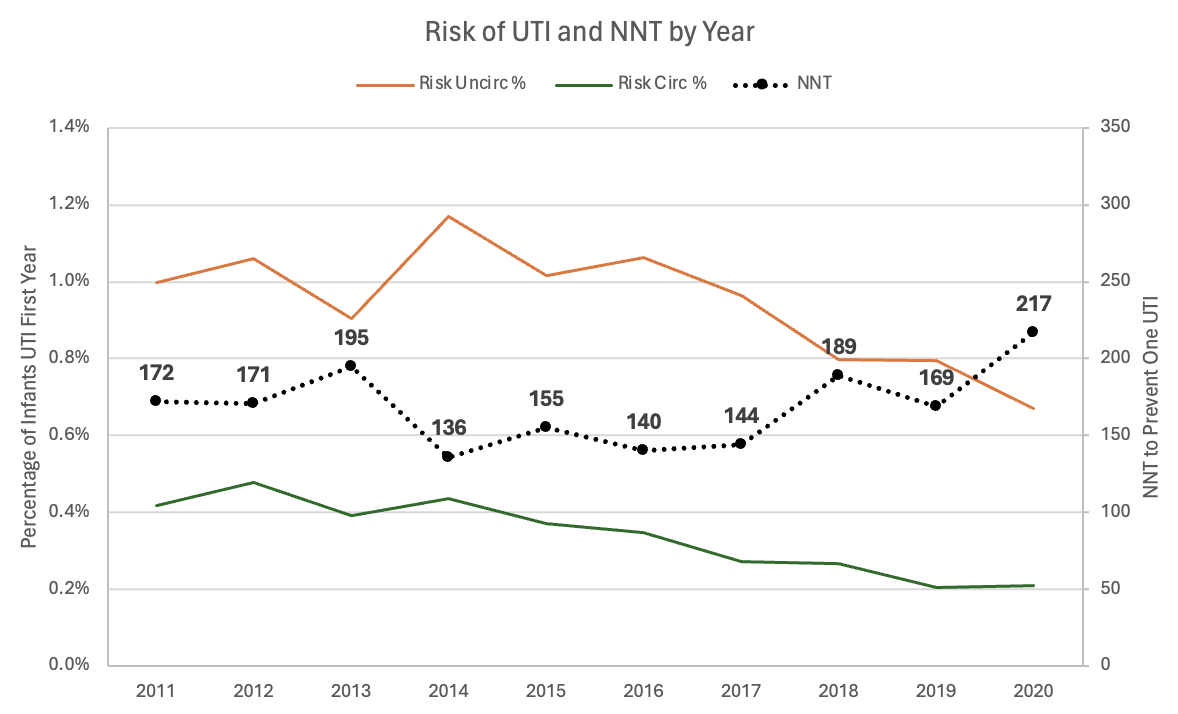
Background: The circumcision number needed to treat (NNT) to prevent urinary tract infection (UTI) is a commonly reported metric used to inform discussions around the benefits of the procedure. NNTs calculated from previous studies have ranged considerably. One meta-analysis reported an NNT of 111 based on pooled estimates from 12 studies. However, most studies reporting NNTs for circumcision were conducted prior to the AAP 2011 UTI Guidelines, which recommended more strict criteria for the diagnosis of UTI (i.e. inclusion of pyuria). Given the potential impact of these stricter criteria on the incidence of UTI, updated NNTs on the efficacy of circumcision in preventing UTI are needed. Objective: To provide contemporary estimates on circumcision frequency and NNT to prevent UTI in infants during the first year after birth. Design/Methods: Retrospective cohort study using the MarketScan Commercial Claims Database which includes healthcare claims from geographically diverse privately insured patients. The cohort included all male infants born between 1/1/2011-12/31/2021 with ≥1 year of continuous insurance enrollment. UTI was defined using ICD-9/10 diagnosis codes plus an antibiotic prescription fill or inpatient antibiotic code within 7 days of diagnosis. Trends in UTI over time were analyzed using a metaregression. NNTs (1/absolute risk reduction) were calculated for each year of study. Results: Among 376,010 male infants, 246,740 (65.6%) underwent circumcision. A total of 2149 (0.6%) infants met criteria for diagnosis of UTI (0.96% uncircumcised vs 0.37% circumcised, p< 0.001). UTI diagnoses decreased during the time period in both circumcised and uncircumcised males (Figure). The absolute decreases were similar in both groups (-.03%/year for circumcised boys, P=.001, -.03%/year for uncircumcised boys, P=.03). The NNT for circumcision to prevent one UTI for the entire time period was 167 and ranged across years from 136-217.
Conclusion(s): The NNT for circumcision to prevent one UTI in a contemporary cohort of male infants is higher than previous reports published prior to the 2011 AAP UTI guidelines. Accurate estimates on the potential benefits of circumcision are essential for informed discussion with families. This higher NNT may be due to adoption of more stringent UTI diagnostic criteria, making the overall absolute risk of UTI lower than pre-2011. However, a decrease in UTI incidence between 2011-20 did not translate into notably increasing NNTs during this time period because the absolute risk decreased similarly between circumcised and uncircumcised boys.

 photo")