Assistant Professor University of Texas at Austin Dell Medical School Austin, Texas, United States
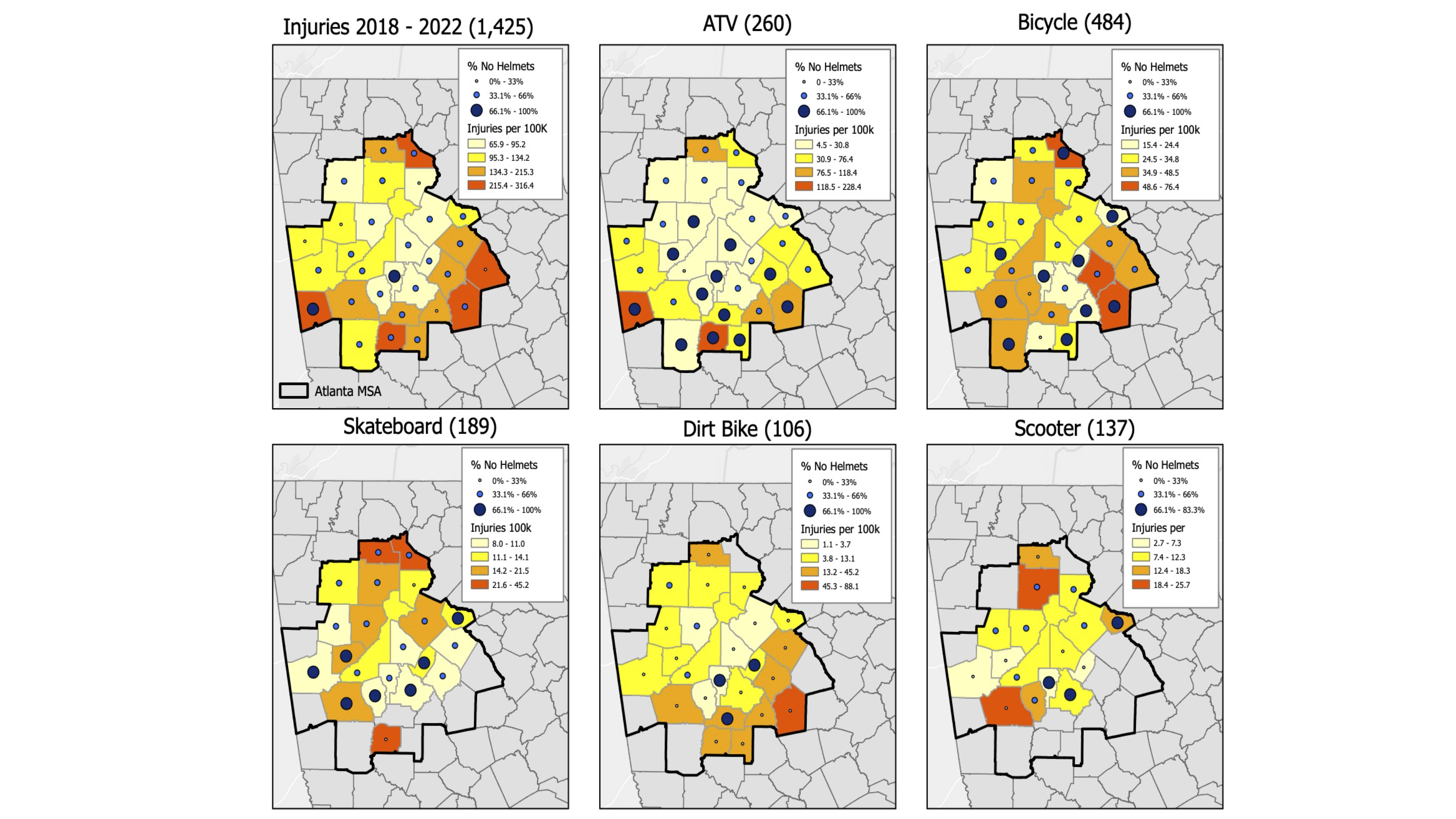
Background: Unintentional injuries, including traumatic brain injuries (TBI) sustained during activities where helmet usage is recommended (AWHUR), are a leading cause of pediatric morbidity and mortality in the US. While advocacy and education are proven measures to address sport safety, community resources in a child’s neighborhood also have a large impact on health and safety. Objective: To evaluate injuries sustained during AWHUR, and correlate with community resources, utilizing the Child Opportunity Index (COI), in conjunction with geographical information system (GIS) mapping. Design/Methods: Utilizing the trauma registry at two pediatric trauma centers in a major metropolitan area from 2018 to 2022, we performed a retrospective chart review and GIS mapping on patients with injuries sustained during AWHUR. The data was analyzed in association with COI data. Inclusion criteria was children 0 to 17 years old who presented with AWHUR-associated injuries. Data extracted from the trauma registry included: mechanism, demographics, insurance status, helmet usage, head injury and Injury Severity Score (ISS). Data was then overlaid with the COI to assess community resources including education, housing, environmental, and socioeconomic factors in relation to injury characteristics. Results: 1425 children were analyzed over the 5-year period. The most common injury mechanisms included: bicycle 34.0%, ATV 18.2%, skateboard 13.3%, scooter 9.2%, and dirt-bike 7.4% (p < 0.001). 381 children were in low or very low COI neighborhoods versus 784 children in high or very high COI neighborhoods. Most patients in very low and low COI were publicly insured, respectively 81.9% and 63.2%; while 65.8% of high COI injured patients were privately insured patients (p < 0.001). Low COI was associated with higher rates of being unhelmeted (78.4%) versus children from very high COI [48.4% (p < 0.001)]. The odds of helmet usage in areas of high COI was 1.96 the odds of helmet usage in low COI. For those injured while wearing a helmet, the odds of higher ISS was 34% less likely than the odds of those who were unhelmeted at time of injury. Additionally, GIS mapping identified specific communities with higher injury rates and lower helmet use in relation to low and very low COI.
Conclusion(s): Children with lower COI were more likely to be publicly insured and unhelmeted at time of injury. Overlapping injury data and COI better identified high risk communities where low resources may contribute to injury severity. This data can be used to inform injury prevention efforts and highlights the importance of community factors.


.png)
.png)