Fellow Physician Lucile Packard Children's Hospital Stanford Palo Alto, California, United States
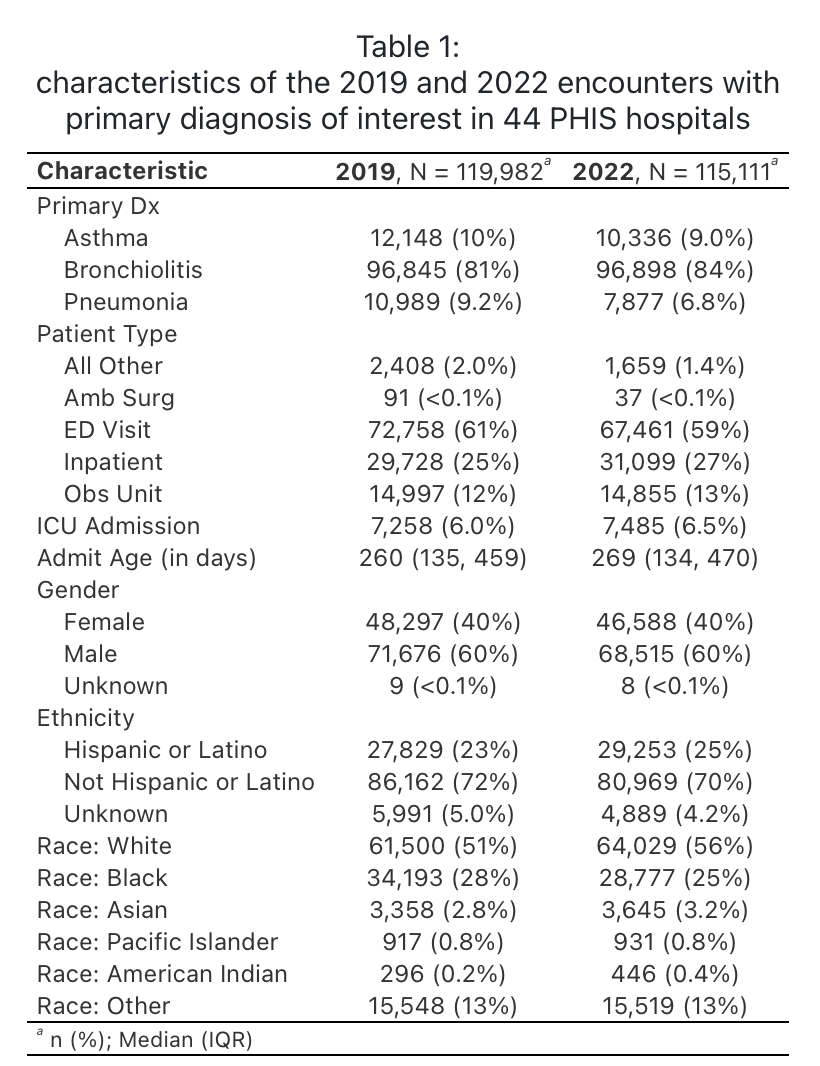
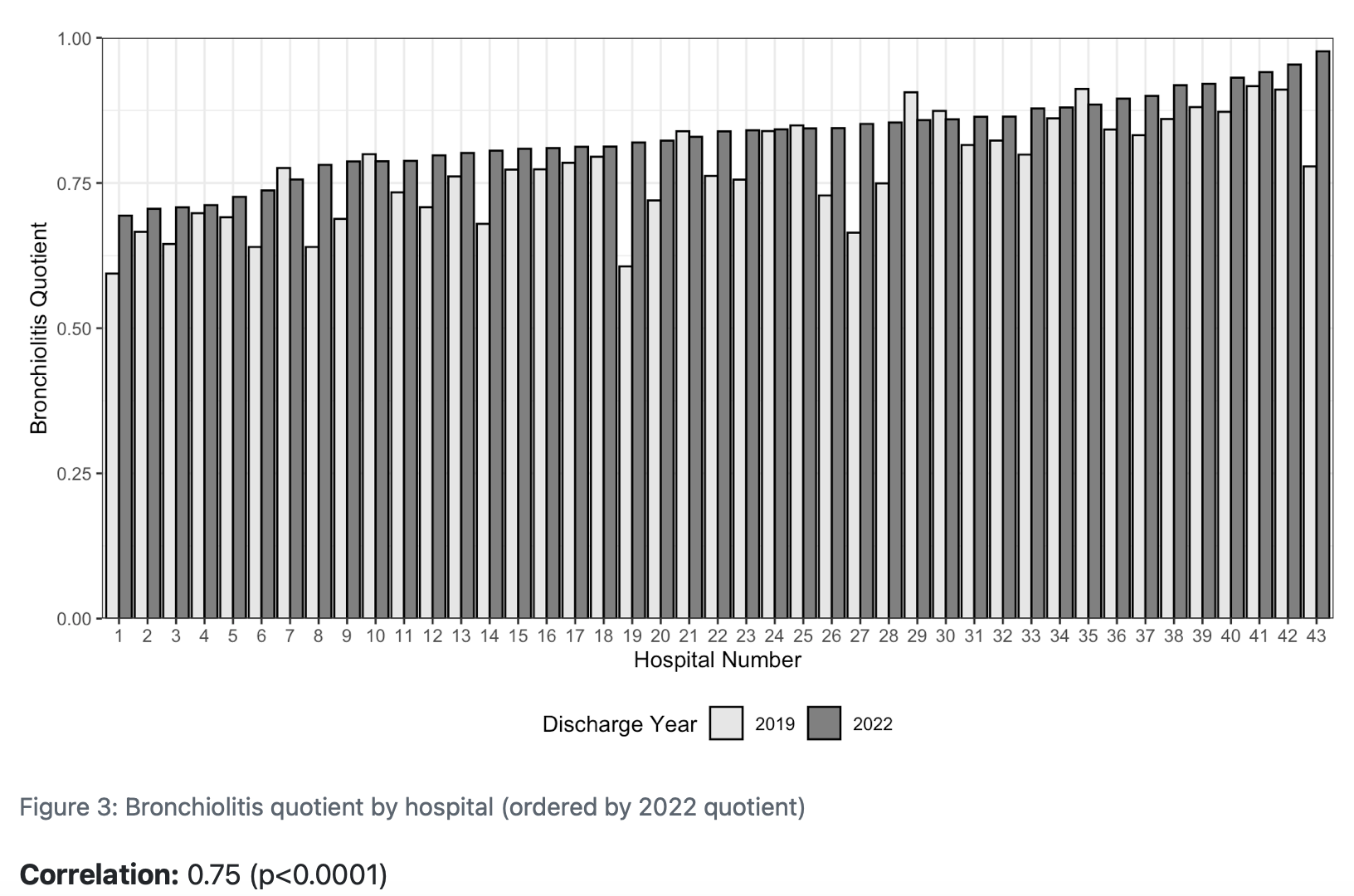
Background: Bronchiolitis is the leading cause of hospitalization in infants and young children. It shares clinical features, such as wheezing and focal radiographic findings, with other respiratory conditions like asthma and pneumonia. As such, children with bronchiolitis might receive alternative respiratory diagnoses. This “diagnostic reclassification” complicates understanding the disease incidence and utilization patterns, particularly when using administrative databases that rely on diagnostic codes for patient identification. Variation in diagnostic coding for children with respiratory conditions has not been well characterized. Objective: We aimed to explore the potential for diagnostic reclassification by examining how the bronchiolitis quotient (BQ), defined as the proportion of bronchiolitis among all cases of bronchiolitis, asthma, and pneumonia, varies by children’s hospitals and over time. Design/Methods: We performed a multicenter retrospective study using the Pediatric Health Information System (PHIS) administrative database containing information from children’s hospitals. Using ICD-10 codes for principal discharge diagnoses, we identified cases of bronchiolitis, pneumonia, and asthma in 2019 and 2022. We excluded patients with complex chronic conditions. Our primary outcome assessed the BQ for all inpatient encounters. In secondary analyses, we explored outcomes in the intensive care unit and the emergency department. Continuous variables were compared using Wilcoxon rank-sum test; temporal trends were analyzed by negative binomial regression models. Results: In 2022, we identified 96,898 cases of bronchiolitis, 7,877 cases of pneumonia, and 10,336 cases of asthma (Table 1) from 44 hospitals. The median BQ for inpatient encounters was higher in 2022 compared to 2019 (.84 vs .78, p=.002) suggesting an increasing proportion of respiratory encounters classified as bronchiolitis. There were no statistically significant differences in the BQ for ED or ICU encounters over time. In 2022 the BQ ranged from .69 to .98 for all inpatient admissions, .61 to .94 for ED visits, and .31 to .96 for ICU encounters across hospitals (Figure 1). Between 2019 and 2022, the BQ for inpatient encounters at individual hospitals was moderately correlated (r=.75, p<.001).
Conclusion(s): The observed variation in the BQ across hospitals and over time is unlikely to be fully explained by regional variation in disease burden. These findings suggest diagnostic reclassification, which may influence estimates of bronchiolitis disease incidence and utilization patterns within administrative databases.

 photo")