Assistant Professor of Pediatrics Monroe Carell Jr. Children's Hospital at Vanderbilt Nashville, Tennessee, United States
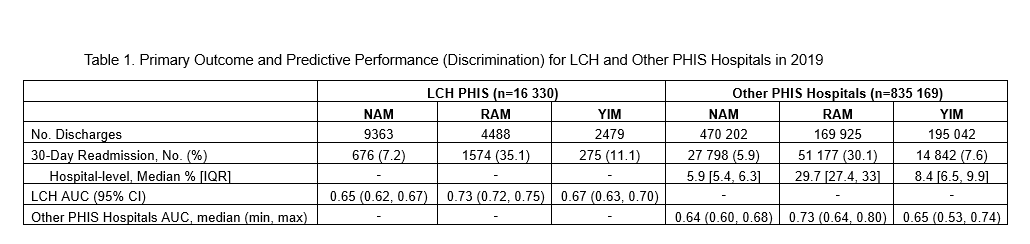
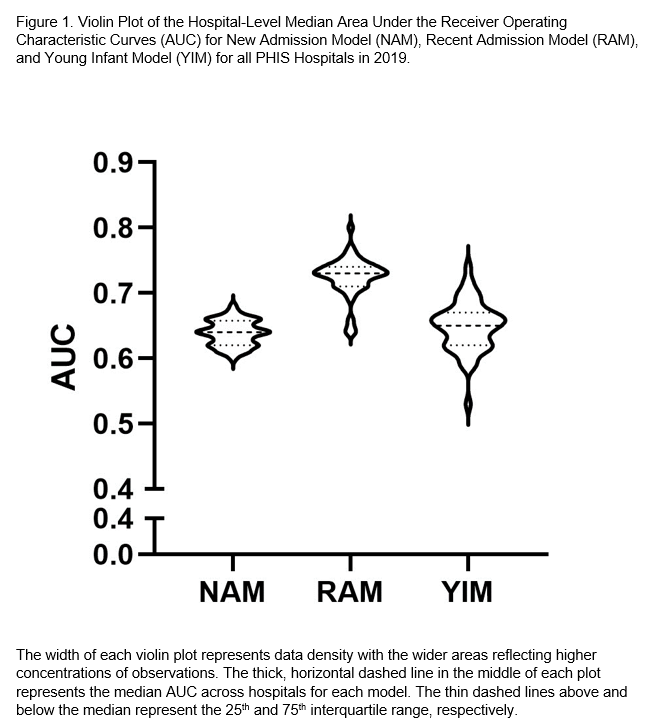
Background: Accurate identification of hospital readmission risk may facilitate safe discharge and avoid preventable readmissions. Objective: To externally validate a suite of models developed at Ann & Robert H. Lurie’s Children’s Hospital of Chicago (LCH) to predict all-cause 30-day pediatric hospital readmissions in a sample of US children’s hospitals. Design/Methods: Model validation was performed using Pediatric Hospital Information System (PHIS) data from 48 US children’s hospitals, including all inpatient and observation encounters for children < 18 years in 2019. All-cause 30-day readmission risk was estimated separately for the 3 LCH models: (1) children ≥ 6 months with ≥ 1 hospitalizations within 6 months (recent admission model [RAM]); (2) children ≥ 6 months with no hospitalizations within 6 months (new admission model [NAM]); (3) all children < 6 months (young infant model [YIM]). Predictors included demographic, clinical, and utilization variables and were identical across each model. Generalized mixed linear regression was used for all analyses. Predictive accuracy of each model was measured for each of the 48 PHIS hospitals and compared against LCH model performance using discrimination (area under the receiver operator curve [AUC], 0.5=discrimination equal to coin flip; 1.0=perfect discrimination). Results: Data from 16,330 LCH encounters and 835,169 other PHIS hospital encounters were included. Readmission prevalence was higher at LCH compared to the average across other PHIS hospitals with variability across the 3 models (Table 1). In each model, the median AUC across PHIS hospitals was nearly identical to the AUC estimated for the corresponding LCH model, although variability in predictive performance was evident across hospitals (Figure 1). None of the models demonstrated ideal discrimination (e.g., AUC >0.8). The RAM demonstrated the best discrimination in both cohorts (AUC of 0.73).
Conclusion(s): Predictive performance of a single center, all-cause 30-day pediatric readmission rule was overall similar when applied in a cohort of 48 peer hospitals across the US. However, discrimination was suboptimal across both cohorts with variable hospital-level performance. Defining reasons for differences in hospital performance and consideration of novel predictors may improve model accuracy, generalizability, and clinical utility.

 photo")