Medical Student Temerty Faculty of Medicine, University of Toronto, Toronto, ON Toronto, Ontario, Canada
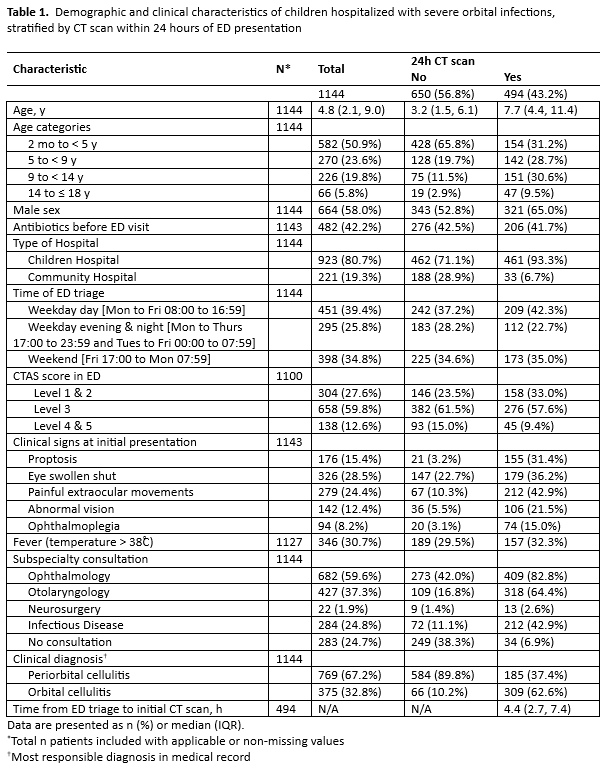
Background: Severe orbital infections require timely diagnosis and treatment to reduce the risk of severe complications such as intracranial abscesses and vision loss. Prior studies have identified variations in the rate and type of diagnostic imaging, but little is known about the factors associated with receiving imaging. Objective: To identify factors associated with computed tomography (CT) imaging within 24 hours of presentation at the emergency department (ED) in hospitalized children with severe orbital infections. Design/Methods: A multicenter retrospective cohort study was conducted in children, ages 2 months to 18 years, who were admitted to 10 Canadian hospitals between 2009 to 2018 with severe orbital infections. Baseline demographics, clinical characteristics and receipt of a CT scan were obtained from hospital medical records. Multivariable modified Poisson regression was used to identify possible factors associated with receiving a CT scan within 24 hours of ED presentation. Results: In 1,144 children (median age 4.8 years) hospitalized with severe orbital infections, 494 (43.2%) received a CT scan within 24 hours of presenting to the ED. Of these, 321 (65.0%) were male and 461 (93.3%) were hospitalized at a children’s hospital. Factors associated with receiving a CT scan within 24 hours of ED presentation included male sex (adjusted relative risk (aRR) 1.18, 95% CI 1.04–1.33), hospitalization at a children’s hospital (aRR 1.80, 95% CI 1.32–2.45), proptosis (aRR 1.39, 95% CI 1.24–1.57) or eye swollen shut (aRR 1.27, 95% CI 1.13–1.43) upon ED presentation, consulted by both ophthalmology and otolaryngology (aRR 3.12, 95% CI 2.35–4.13) or by either ophthalmology (aRR 2.19, 95% CI 1.66–2.90) or otolaryngology (aRR 2.66, 95% CI 1.84–3.86). Children ages 2 months to < 5 years, however, were less likely to receive a CT scan within 24 hours of ED presentation (aRR 0.63, 95% CI 0.53–0.74). Use of antibiotics prior to ED visit, time of ED presentation (weekday day, weekday evening or night, weekend), Canadian Triage and Acuity Scale (CTAS) score, temperature >38˚ C, WBC or CRP levels were not associated with receiving a CT scan within 24 hours.
Conclusion(s): In hospitalized children with severe orbital infections, subspecialty involvement by ophthalmology and/or otolaryngology is the strongest predictor of receiving a CT scan within 24 hours of ED presentation, with children < 5 years less likely to have diagnostic imaging. Further research is needed to understand the impact of diagnostic imaging on management.

 photo")
.png)