Clinical Fellow The Children's Hospital at Montefiore Lynbrook, New York, United States
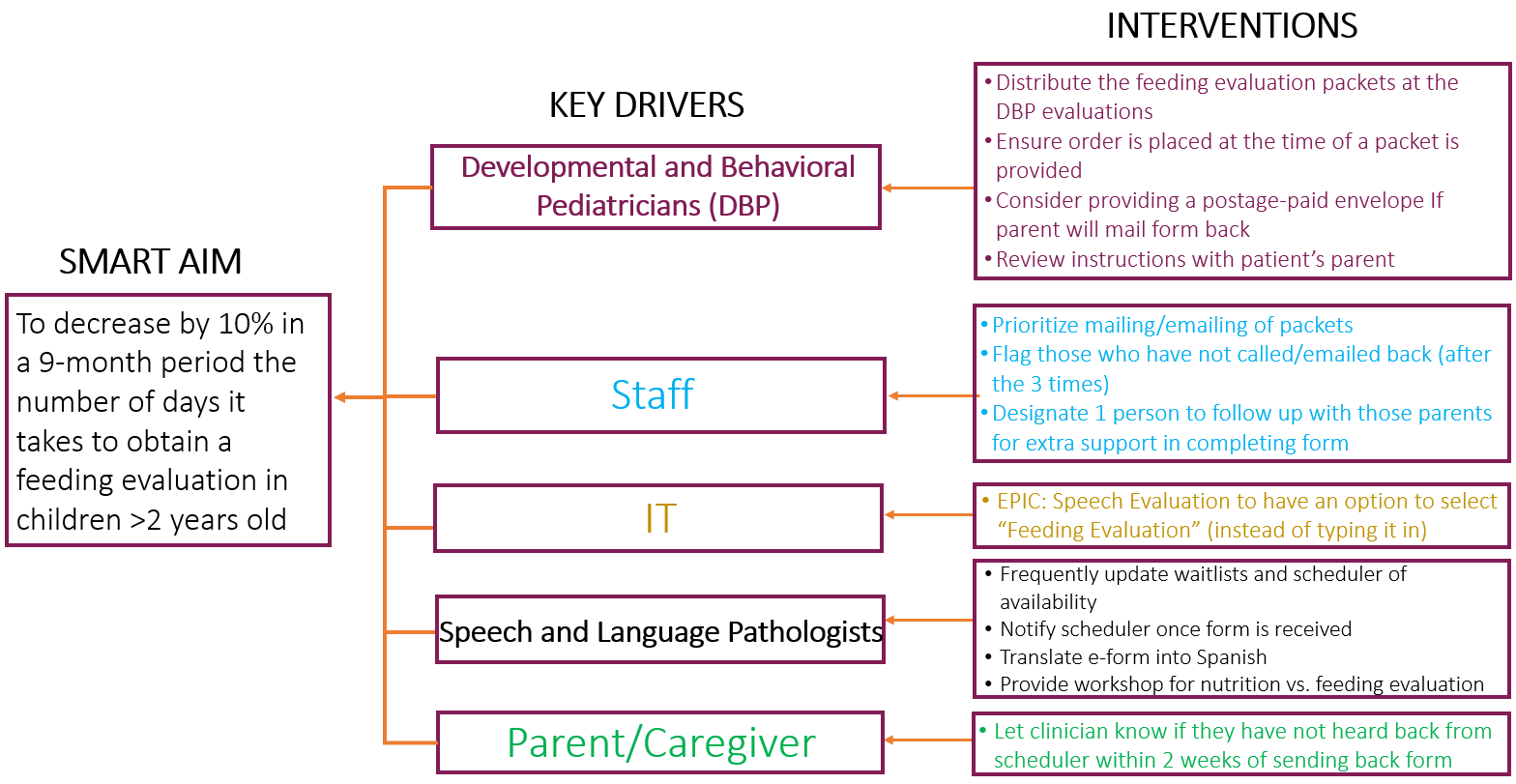
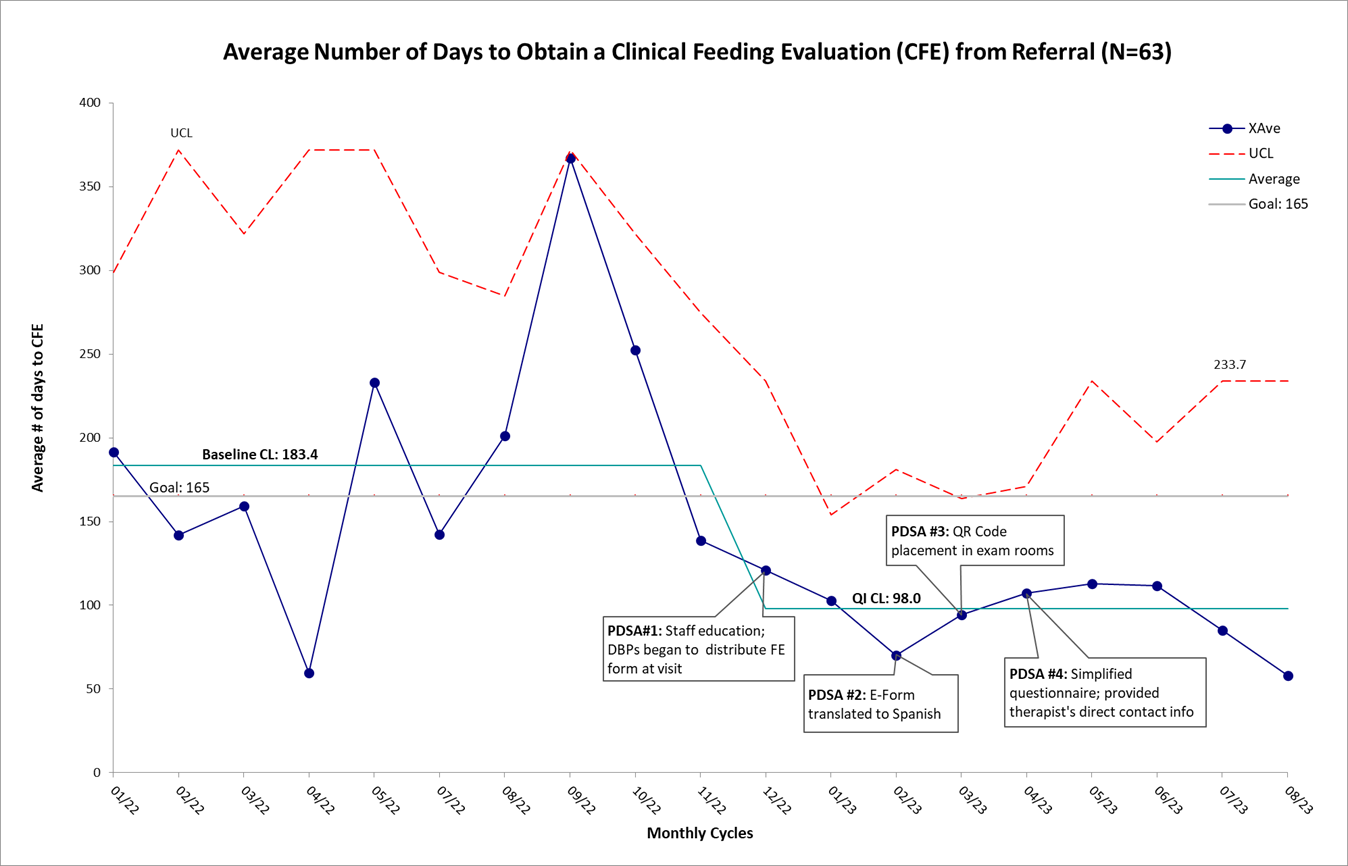
Background: Children with developmental disabilities (DDs) are at increased risk for developing feeding problems and secondary nutritional deficiencies compared to typically developing children. Obtaining a clinical feeding evaluation (CFE) helps characterize those most at risk for feeding and nutrition problems, and determine which patients need feeding therapy. The process of obtaining a CFE from initial referral can be lengthy. This in turn affects early identification and treatment of feeding challenges and can result in restrictive eating habits, maladaptive behaviors, negative mealtime experiences, and skill level deficits. Therefore, it is important to identify barriers that impact this process to improve accessibility and develop a more expeditious process. Objective: To reduce the time needed to complete a CFE from initial referral at an ethnically diverse, urban multidisciplinary university-affiliated developmental center using quality improvement (QI) techniques and to identify barriers in the process. As children ≤2 years are already prioritized at our center, we focused on children >2 years. Design/Methods: QI methodology was implemented. The SMART aim was to decrease the number of days it takes to obtain a CFE for children >2 years by 10% in a 9-month period. The primary outcome was the number of days between CFE referral to evaluation appointment. Data collected includes a baseline period (01/22-11/22) and four Plan-Do-Study-Act cycles (12/22-08/23). In 11/2022, we defined our project aim, assembled a team of key stakeholders including developmental and behavioral pediatricians, speech and language pathologists, schedulers, and developed cause-and-effect and key driver diagrams to further guide our interventions (Figure 1). Interventions consisted of initial staff education on the process of obtaining a CFE, distribution of feeding questionnaires (FQs) at the time of referral, development of Spanish/English online FQs, development of FQ QR codes and placement in exam rooms for greater accessibility, and simplification of the FQ. Results: The baseline period showed that it took children >2 years a mean of 183 days to obtain a CFE from initial referral (n=32). Following the start of the QI project and four PDSA cycles (n=31), special cause variation was achieved resulting in a center-line shift to a mean of 98 days, indicating a 47% reduction (Figure 2).
Conclusion(s): After implementation of four PDSA cycles, the team was successful in reducing the time-to-CFE in children >2 years. Efforts are being developed to promote the sustainability of this improvement and further address barriers.

 photo")