Resident University of Colorado School of Medicine Aurora, Colorado, United States
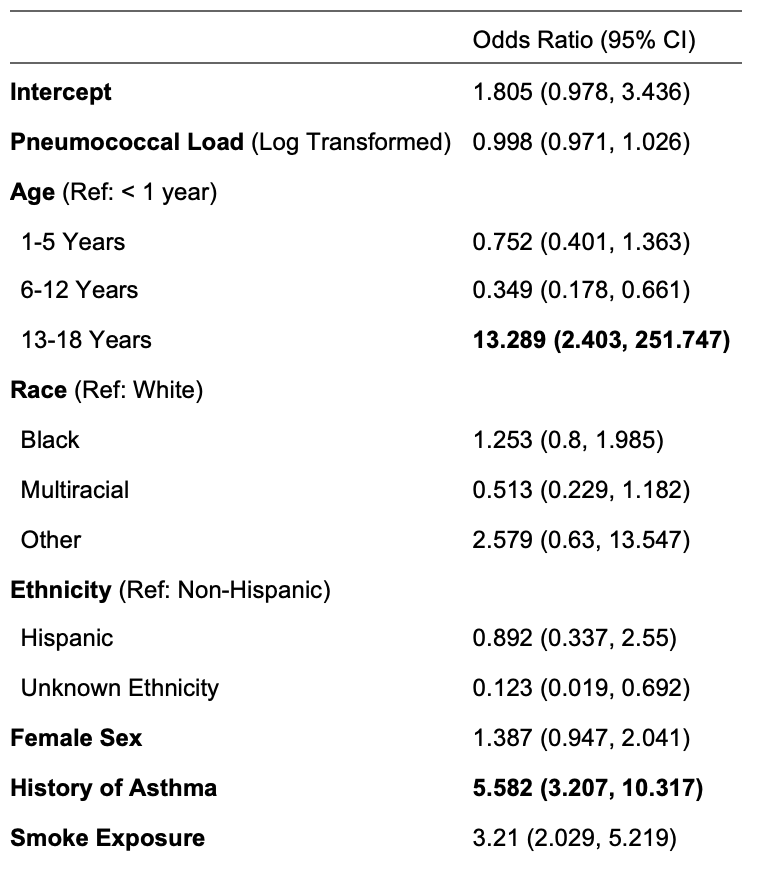
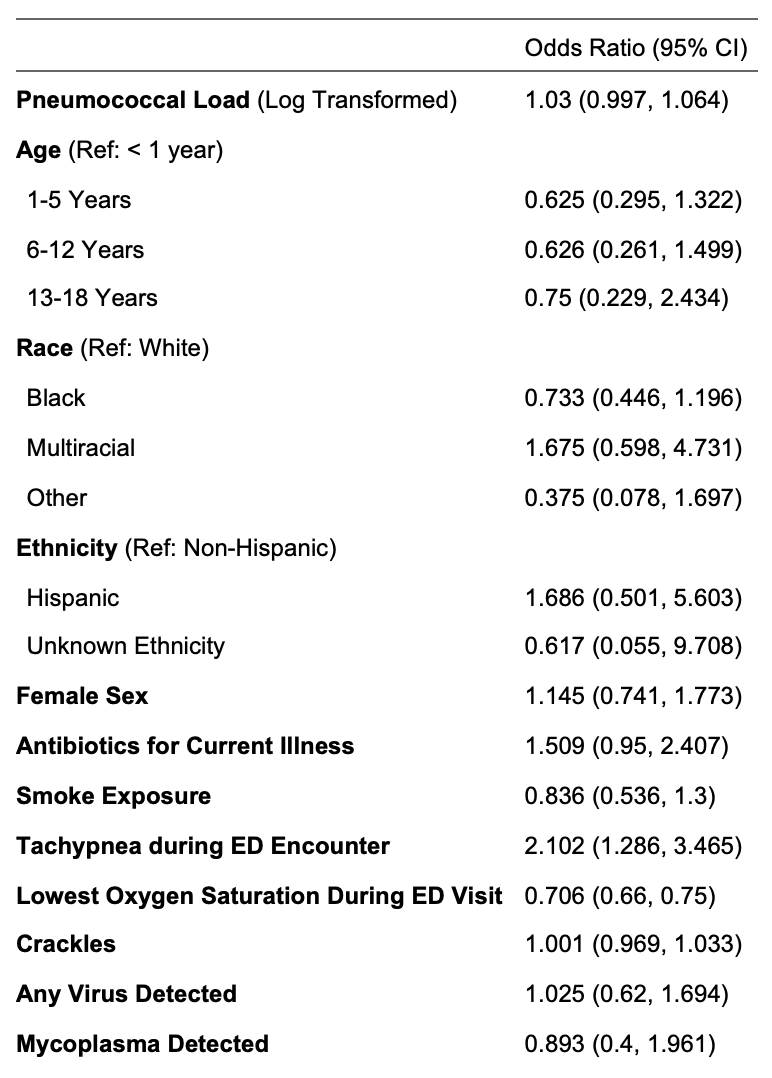
Background: Pneumococcal colonization is common among children. The relationship between pneumococcal colonization and suspected community-acquired (CAP) in children is poorly characterized. Objective: To identify risk factors associated with nasopharyngeal pneumococcal carriage and elucidate the utility of nasopharyngeal pneumococcal carriage as a predictor of suspected CAP and severity of CAP. Design/Methods: We conducted a case-control study to evaluate nasopharyngeal pneumococcal carriage in children with and without suspected CAP. Cases were defined as previously healthy children aged 3 months to 18 years old who presented to the emergency department with signs and symptoms and who received a chest radiograph (CXR) for suspicion of CAP. Controls were defined as healthy children without respiratory infections from the community. A nasopharyngeal swab was obtained from each child and assayed for lytA, a gene fragment of Streptococcus pneumoniae. Pneumococcal load was log-transformed to achieve normality. Three models were created: 1. multivariable linear regression to assess for an association between potential risk factors (age, race, ethnicity, sex, history of asthma and smoke exposure) and pneumococcal load; 2. multivariable logistic regression to assess the association between pneumococcal load and suspected CAP (Table 2); and 3. A multivariable ordinal logistic regression to assess for association between pneumococcal load and severity of suspected CAP (Table 3). Severity of suspected CAP was defined as mild (discharged from the emergency department), moderate (inpatient hospitalization), and severe (requiring intensive care or evidence of severe sepsis). Results: We included 474 cases and 185 controls, 51.4% (339) were between 1-5 years old, and 26.1% (172) had a history of asthma (Table 1). Pneumococcal load was negatively associated with increasing age. For every 5.706 decrease in log base 2 transformed pneumococcal load, age increased from under 1 year old to 6-12 years of age and to 13-18 years of age for every 6.824 decrease in log base 2 transformed pneumococcal load. There was no statistical association between pneumococcal load and race, ethnicity, sex, history of asthma, or history of smoke exposure There was no statistical association between pneumococcal load and suspected CAP versus control (Table 2) and also no statistical association between pneumococcal load and CAP severity (Table 3).
Conclusion(s): Pneumococcal load decreased with age among children in our study. Pneumococcal load was not associated with the suspicion of CAP and was not a useful tool for predicting the severity of CAP.


.png)