Assistant Professor Jichi Medical University Shimotsuke, Tochigi, Japan
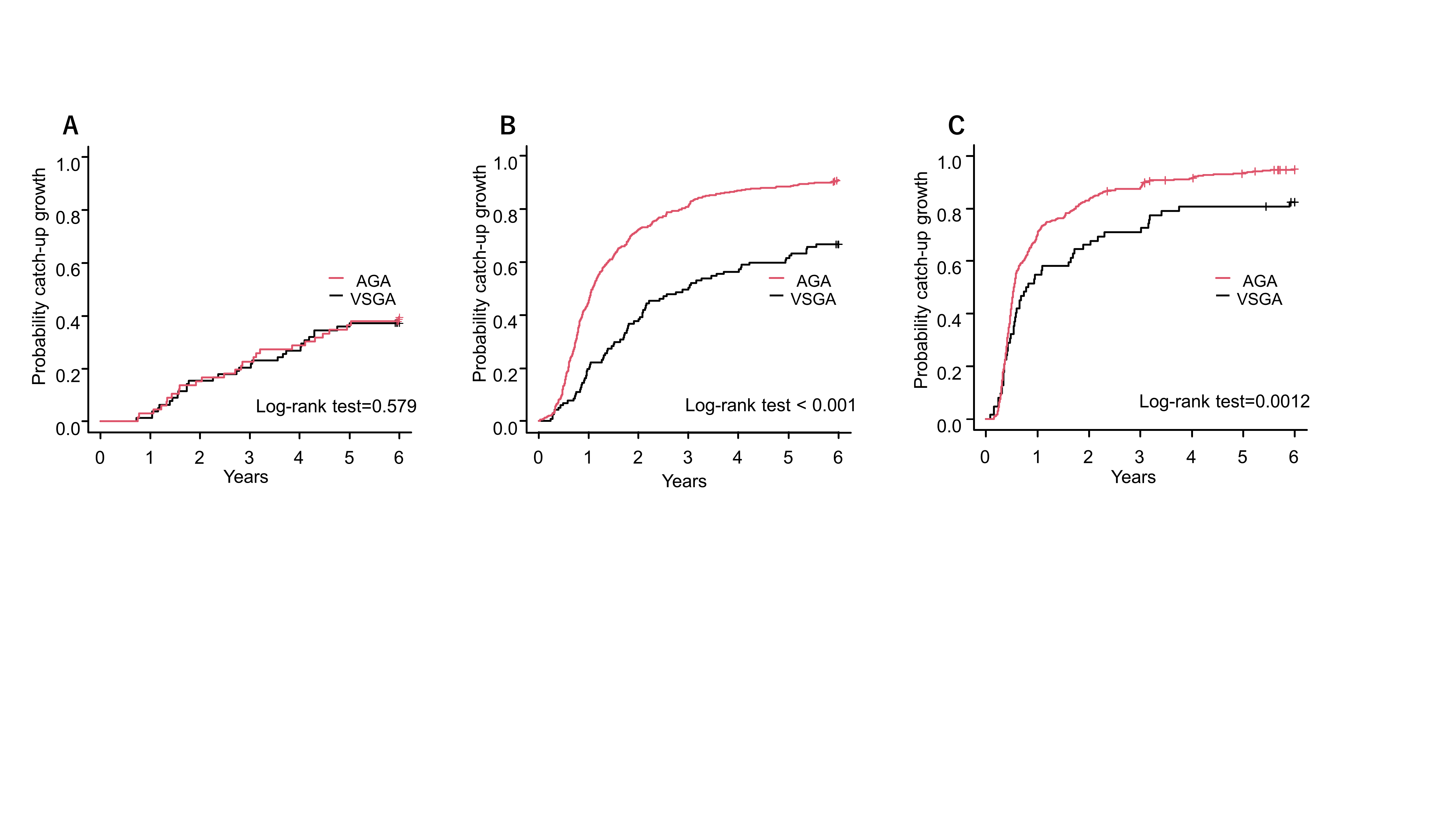
Background: Small-for-gestational age (SGA) infants have a risk for long-term growth impairment. The more severe the fetal growth retardation, rather than the lower birth weight (BW), the higher the risk of subsequent growth failure. Among SGA, long-term growth trajectory of smaller SGA with BW < -3 standard deviation (SD) remains unknown. Objective: To describe long-term weight growth in very low birth weight infants with BW < -3SD (very SGA: VSGA), and to explore the determinants of catch-up (CU) growth in this population. Design/Methods: This is a secondary analysis of “The research on the establishment of growth and developmental assessment methods for low birth weight infants” (Health Labour Sciences Research Grant, 21DA1005). This multicenter retrospective cohort study included infants with a BW < 2500 g born between 2012 and 2016 in 70 NICU in Japan. The clinical and anthropometric data were collected from medical records, and/or photos uploaded by parents. The present analysis included infants with BW < 1500 g without congenital disorders. Participants were divided into 3 groups according to BW, < 500 g (group A), 500-999 g (group B), 1000-1499 g (group C). CU (exceeding -2SD by Japanese standards) rates of weight up to age 6 were compared between appropriate-for-gestational age (AGA) and VSGA. The clinical factors between CU and non-CU group in VSGA were compared. Results: A total of 144, 718, and 675 in group A, B, and C, respectively, were included in this analysis. The background data of AGA and VSGA in each group were shown in Table 1. Using Kaplan-Meier curve, the CU growth of weight up to 6 years for each group was shown in Figure 1. Unlike group B and C, no significant difference was found between AGA and VSGA in group A. CU rates of weight in VSGA at 3/6 years were 16.7/35.9%, 39.3/56.4%, and 59.7/77.4% in group A, B, and C, respectively. In comparison between CU and non-CU group in VSGA, BW SD score (SDS) was significantly lower in non-CU group of group B at age 3 and 6 and C at age 3, but not in group A. The rate of growth hormone treatment for short stature was significantly higher in non-CU group of group A at 6 years, B at 3 and 6 years, and C at 3 years.
Conclusion(s): CU rates were significantly lower in VSGA with BW < 500-1499 g compared with AGA. In infants with BW < 500 g, both AGA and VSGA had long-term growth retardation with a CU rate of < 40% at age 6, with no significant differences. There were few clinical factors affecting CU growth in VSGA other than SDS of BW.

.png)