Associate Clinical Professor of Pediatrics UC San Diego San Diego, California, United States
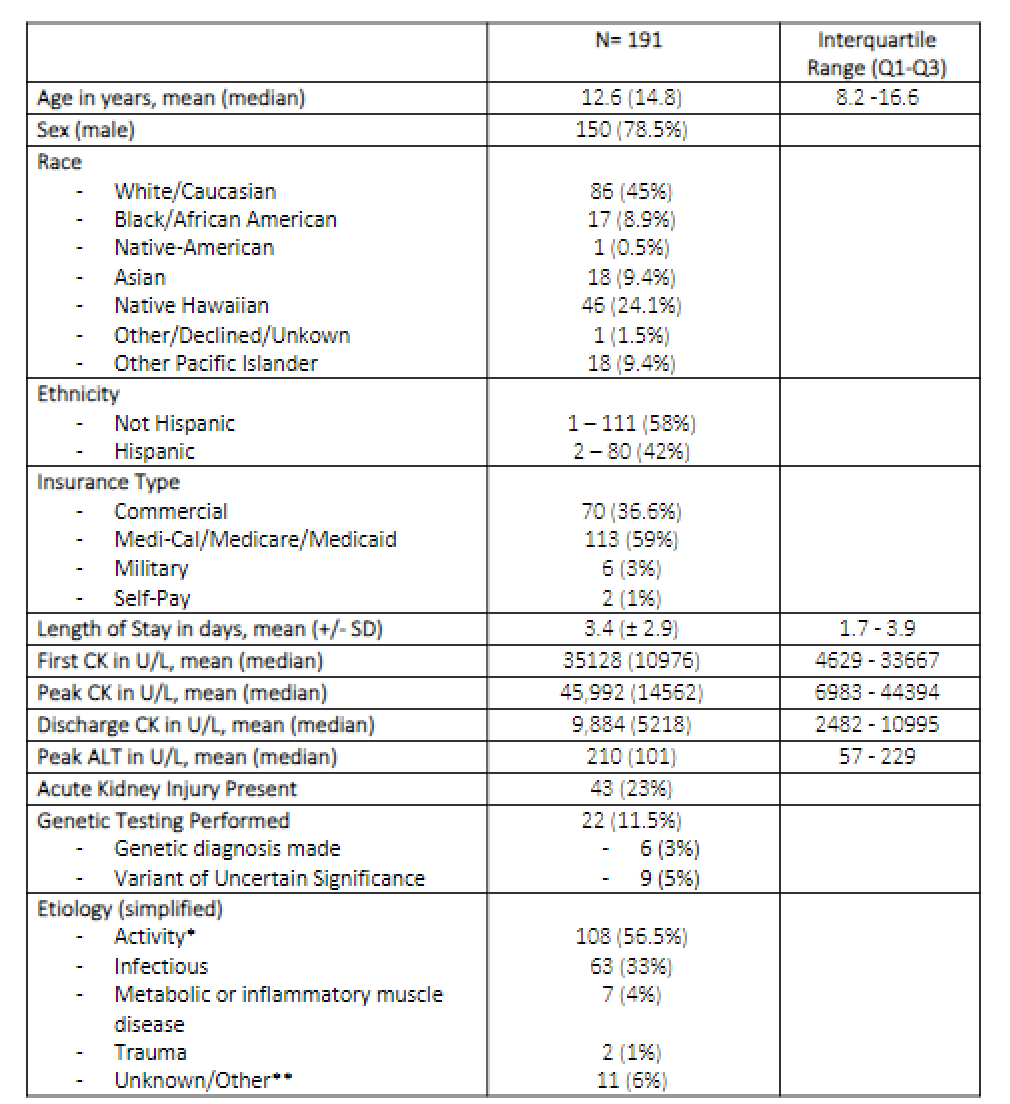
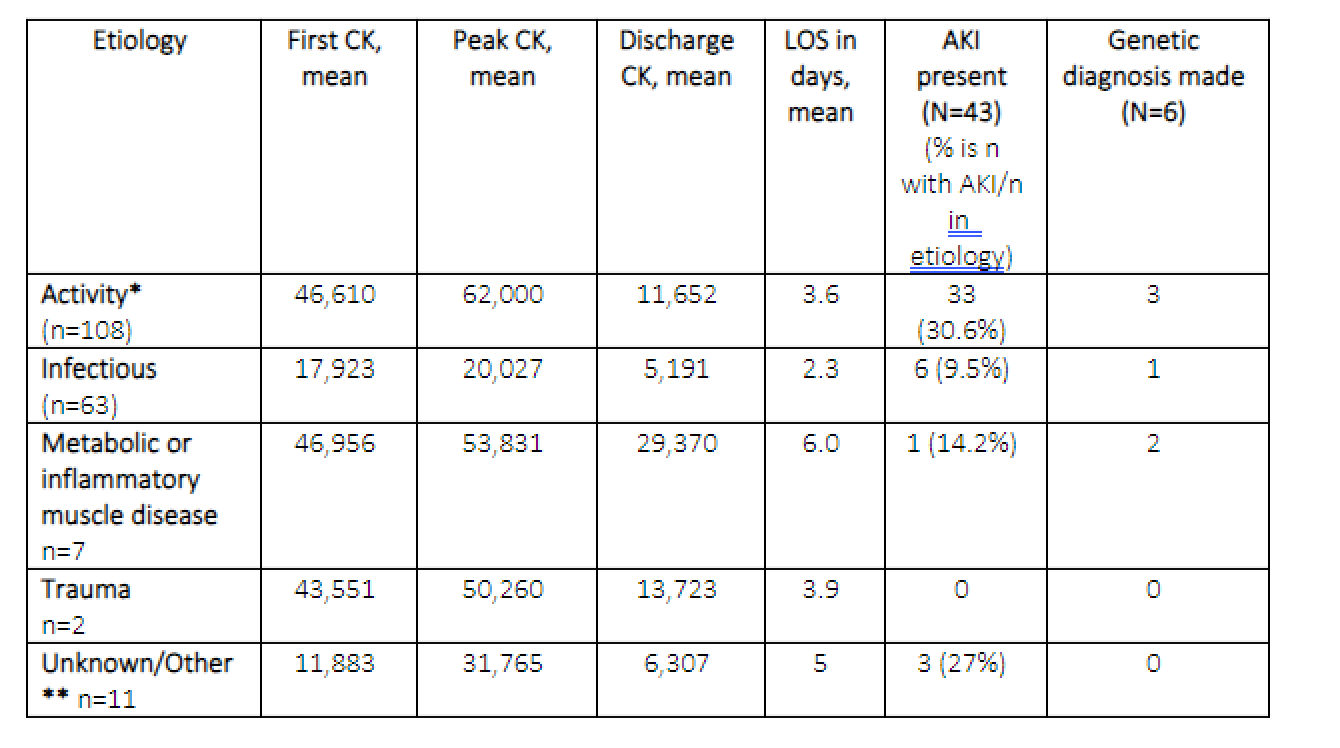
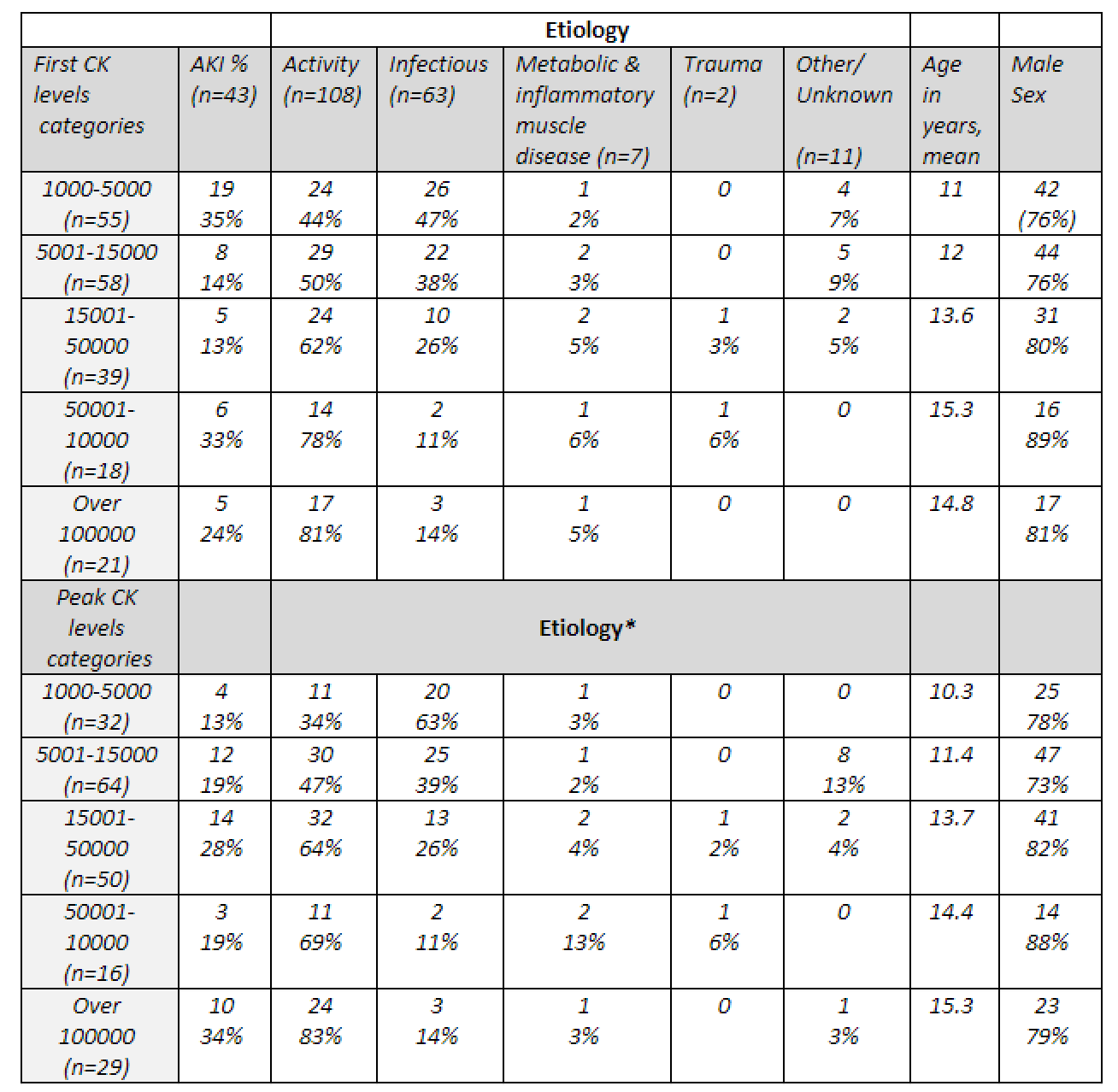
Background: Rhabdomyolysis is the destruction of skeletal muscle cells resulting in the release of contents into the bloodstream. Children are often hospitalized out of concern for the development of acute kidney injury (AKI). There is a paucity of evidence to guide risk evaluation of AKI, correlation with different causative etiologies, and management of children hospitalized with rhabdomyolysis. Objective: To describe the clinical characteristics of hospitalized children with rhabdomyolysis including AKI Design/Methods: We conducted a retrospective chart review of subjects less than 19 years old with a discharge diagnosis of rhabdomyolysis that were hospitalized at our pediatric tertiary care hospital from 2012 to 2022. Inclusion criteria was a creatinine kinase (CK) level > 1000 U/L. For patients with multiple admissions, the index admission was used for analysis. Patients with prolonged hospitalization due to factors other than rhabdomyolysis or diagnoses that confounded diagnosis of AKI were excluded. Data was obtained through manual review after automatic retrieval from the electronic medical record with subject identification via hospital discharge diagnoses using the ICD-9 or 10 codes for rhabdomyolysis (728.88 and M62.82). Results: Of 191 patients, 11 had >1 admission for rhabdomyolysis. 79% of patients were male with an average age of 12.6 years. The average length of stay was 3.4 days with 7% (n=13) of patients requiring PICU admission. The median peak CK value was 14,562 with the median CK at discharge of 5,218 (Table 1). 43 (23%) had AKI, the majority (33, 77%) were in the activity etiology group. The activity group included patients with seizures, excessive exercise and severe agitation. On average patients in the activity group had the highest peak CK levels and 31 % in this group presented with AKI (table 2). Overall, patients with AKI had a longer LOS (5 vs 2.9 days without AKI). There were significant differences when comparing peak CK level versus etiology (Table 3). 22 patients received genetic testing, of those 6 had a genetic diagnosis identified. No patients required dialysis and there were no deaths from rhabdomyolysis, or its sequelae reported. Only 2 patients had a related readmission within 30 days, and 4 patients had a related ER visit within 30 days after discharge.
Conclusion(s): This is the largest reported study of hospitalized children with rhabdomyolysis in the US. Most patients with AKI were in the activity group. More evidence is needed to stratify risk groups and guide the management of children hospitalized with rhabdomyolysis.