Resident Doctor Boston Children's Hospital Boston, Massachusetts, United States
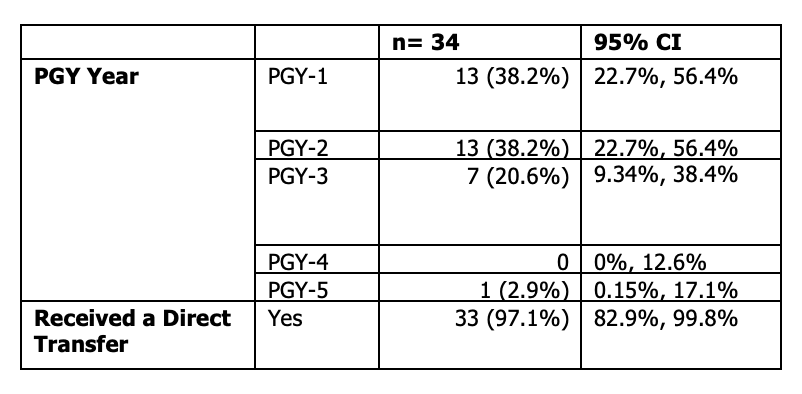
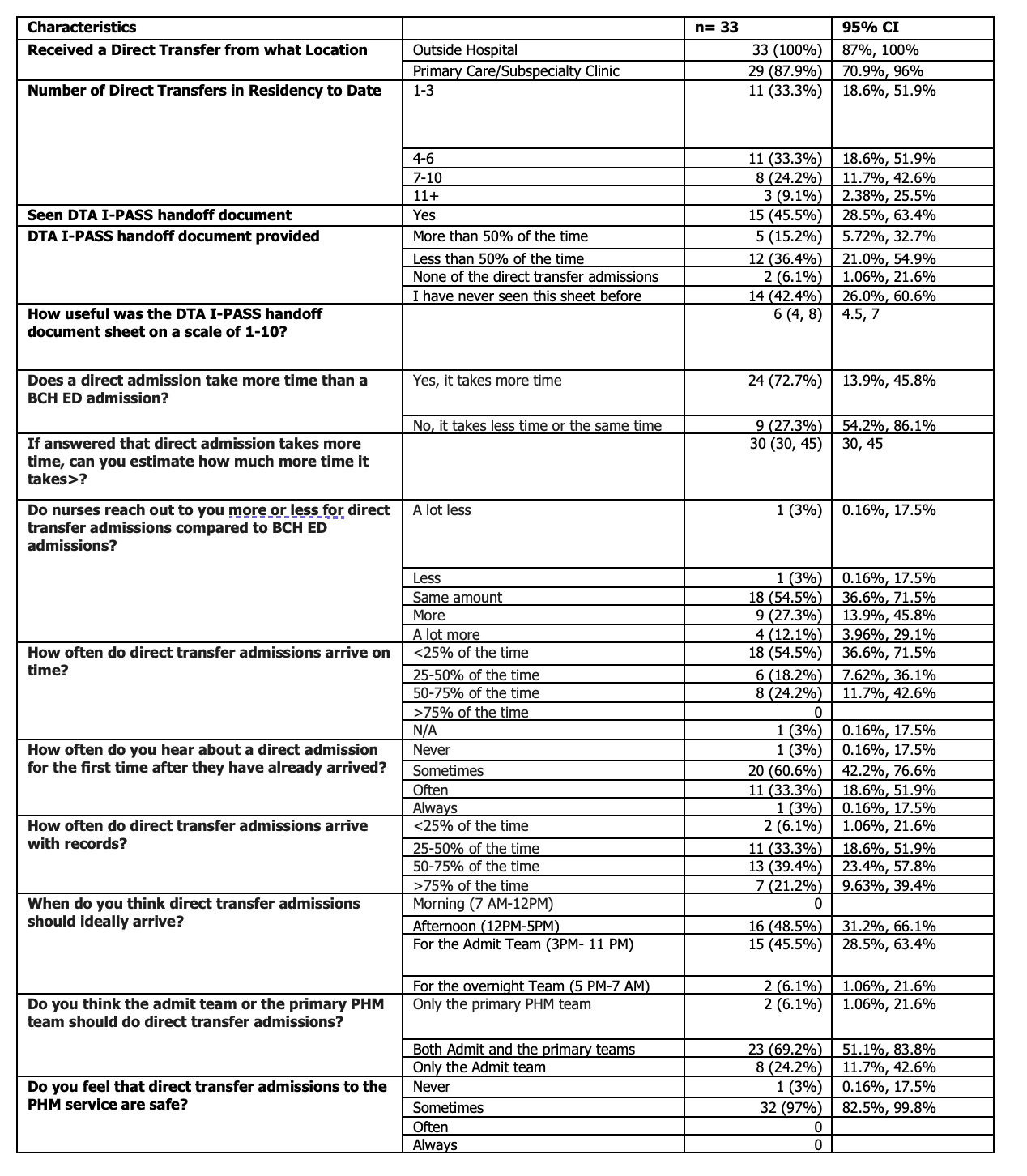
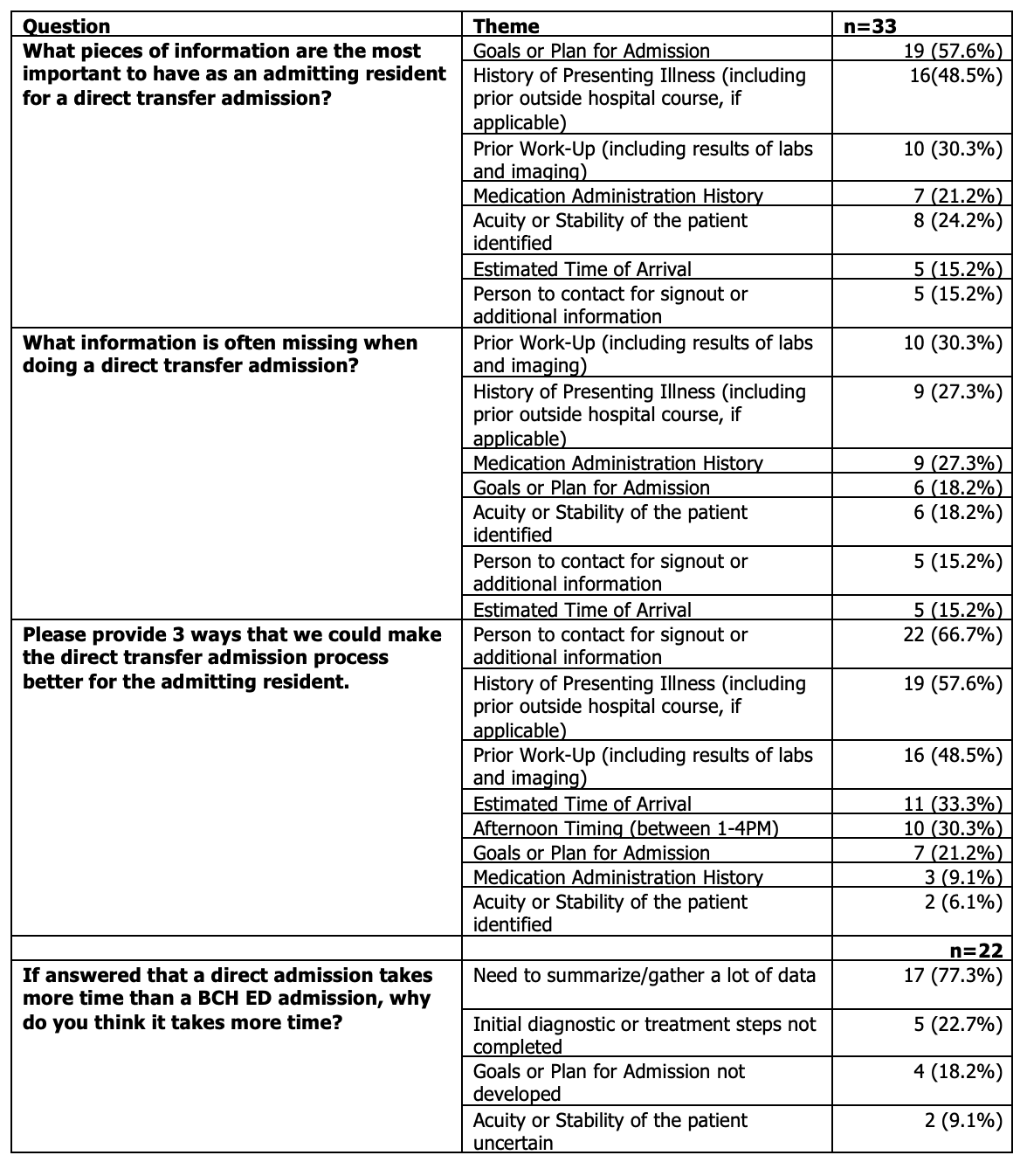
Background: Direct transfer admissions (DTAs) allow patients to be directly admitted from an outside hospital or clinic to the inpatient floor. While local QI work has been done to try to make this process safer and more protocoled for the accepting team, including adoption of I-PASS signout handoff document, there are still pain points related to communication, acuity, and safety. The resident team often express poor satisfaction compared to admissions through the Emergency Department. Objective: To better understand the resident experience related to DTAs, and to identify areas for improvement and resident-proposed solutions. Design/Methods: A survey was sent to the residents who had completed at least 1 year of residency in a large tertiary children’s hospital. The survey includes questionaries of DTA processes and resident satisfaction measures either by categorical (Likert scales) or continuous variables. Descriptive summaries of the responses are presented as percentages with 95% confidence intervals (CI) for categorical outcomes and median with a Wilcoxon test 95% CI for continuous outcomes. Short answer responses were coded using thematic analysis. Results: Among the 33 eligible residents who completed the survey (Table 1), 33% had received more than 6 DTAs. 73% of respondents stated that DTAs take more time than a typical admission. 97% of residents have had at least one DTA where the patient has already arrived to the floor before they were made aware an admission was coming, and 39% report that less than half of the time patients arrive with records from the outside facility. When asked what pieces of information were most important for the admitting resident to have, common themes included goals or reason for admission (58%), history of presenting illness (including outside hospital course) (49%) and prior workup (30%). Lastly, when asked about ways to make the DTA process better for the admitting resident, the top theme was having a person to contact for signout or additional information (67%) (Table 3).
Conclusion(s): While strides have been made in recent years to improve the safety of DTA process, the experience of the admitting resident continues to need improvement. This survey highlights the need for greater communication between the outside facility and the admitting resident, including documentation of prior work-up, clearly outlined proposed plan and a person to contact for signout or additional information. This data will be used to improve the content and usage of our internal I-PASS handoff document, which could be adapted to other facilities to optimize the DTA process.