Medical Student Emory University School of Medicine Atlanta, Georgia, United States
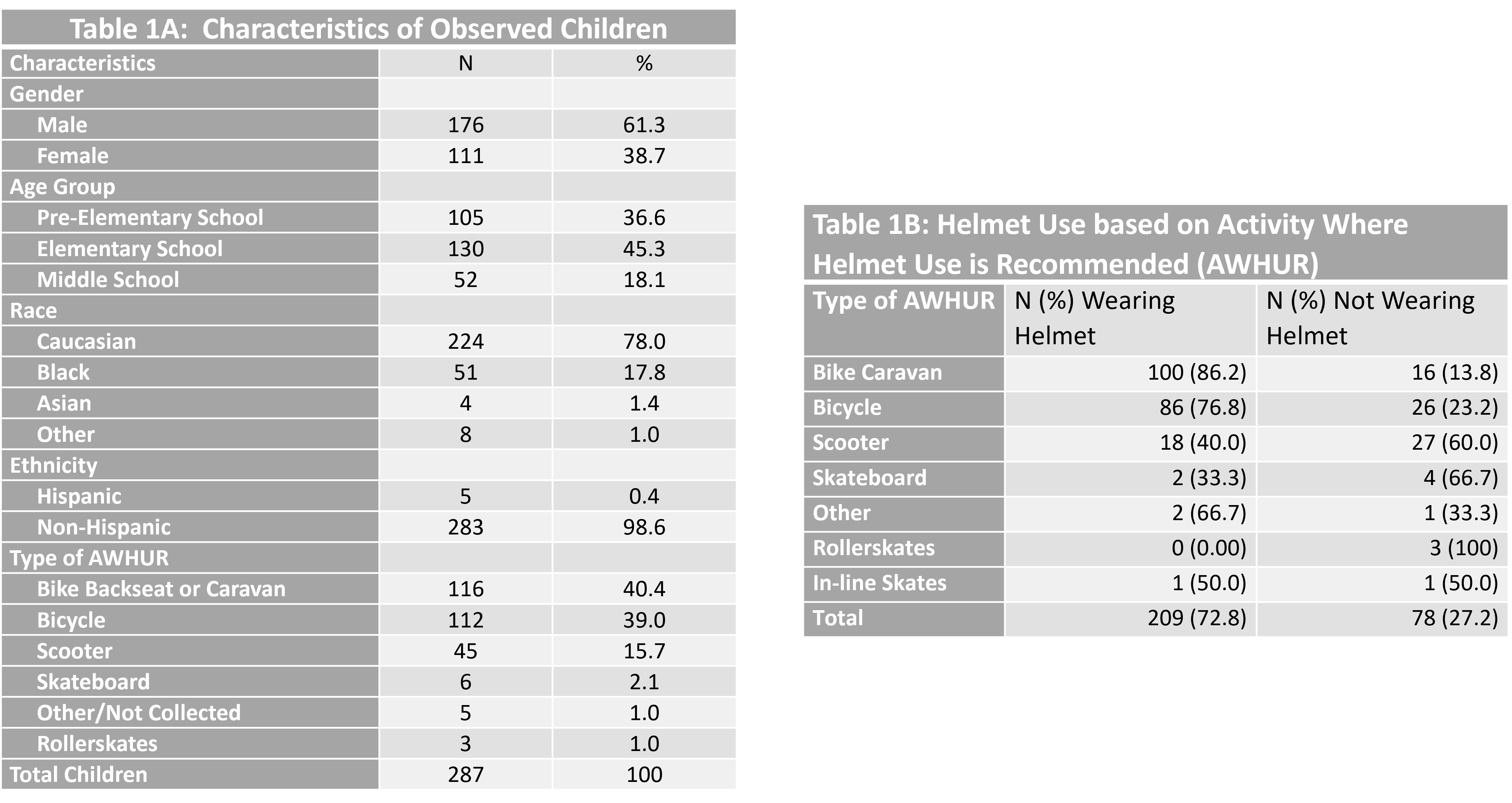
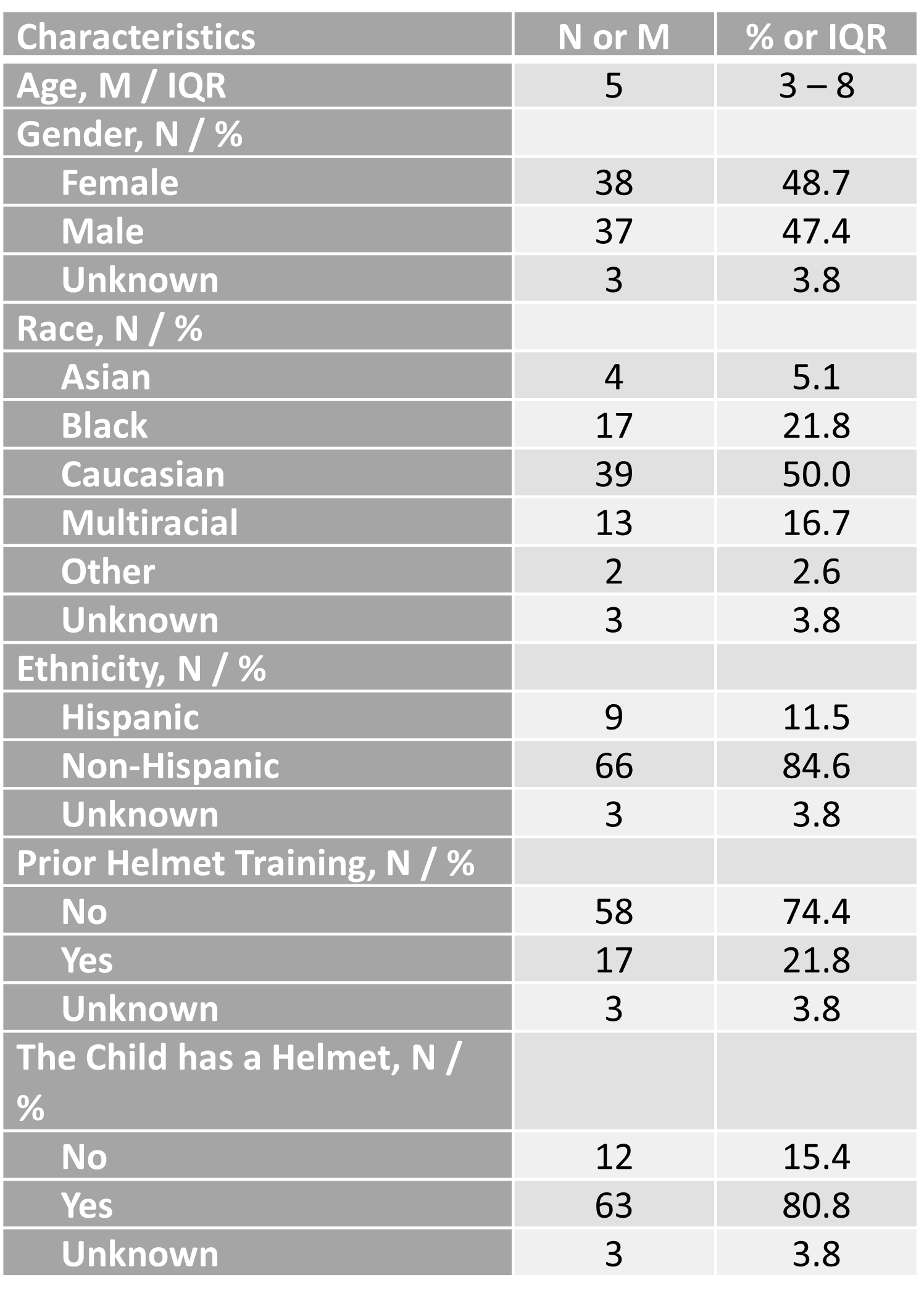
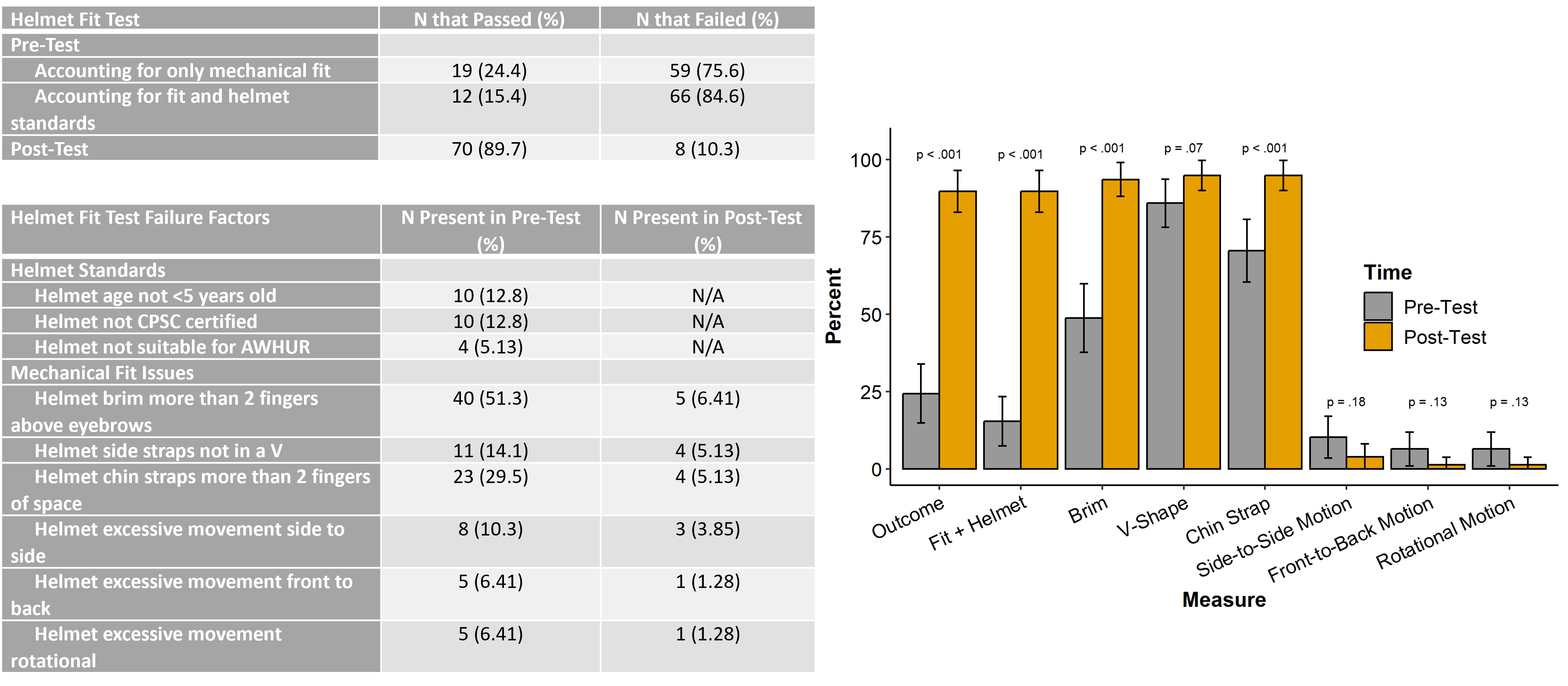
Background: Pediatric traumatic brain injuries from activities for which helmet use is recommended (AWHUR) can be mitigated by use of an appropriately fitting helmet. However the rate of appropriate helmet use during AWHUR on dedicated pedestrian/bicycle paths may vary, and the efficacy of brief education regarding helmet fit is unknown. Objective: To evaluate helmet use of children participating in AWHUR on a dedicated bike/pedestrian path and to evaluate the effect of a brief educational intervention on helmet fit. Design/Methods: In this study’s observational arm, we observed children participating in AWHUR and recorded sex, race, estimated age, type of AWHUR, and helmet use. In the interventional arm, guardian/child pairs were asked to complete a pre/post assessment. Participants completed a survey on demographics and helmet use. Educators assessed helmet fit after the caregiver put their child’s helmet on or supervised their child’s own helmet placement. Helmet fit was assessed based on chin strap and side strap placement, helmet brim height, and helmet movement greater than 1 inch in any direction. Helmet standards were also assessed for age, certification, and AWHUR suitability. Any single incorrect element resulted in a fail. Then, an educator demonstrated proper helmet fit. After loosening straps and removing the helmet, guardians fit it on their child a second time; this post-education assessment was recorded, with additional feedback if needed. The pre- and post-test values were compared using McNemar’s test and are reported with p-values. Results: Of the 287 children in the observational arm, most were engaged in bicycling (39.0%) or riding in a bike seat or caravan (40.4%) (Table 1). Overall helmet use was 72.8% with rates varying by activity. In the interventional arm, even though 80.8% of 78 guardian/child dyads endorsed helmet ownership, only 24.4% demonstrated appropriate helmet fit pre-intervention; this fell to 15.4% when accounting for helmet standards. Post-intervention, helmet fit improved to 89.7% (p < 0.001) (figure 1). The most common areas of poor fit pre-intervention included helmet brim (51.3%) and chin strap placement (29.5%); post-intervention this improved to 93.6% and 94.9% respectively (p < 0.001).
Conclusion(s): Even though pediatric helmet use during AWHUR on a dedicated pedestrian/bicycle path was high, appropriate helmet use and fit was suboptimal. A brief educational intervention significantly improved helmet fit immediately after education. Further study on whether improvements in helmet fit were retained over time is warranted.

.jpg "Jordan Couceyro (he/him/his) photo")