Assistant Professor Michigan State University College of Human Medicine Lansing, Michigan, United States
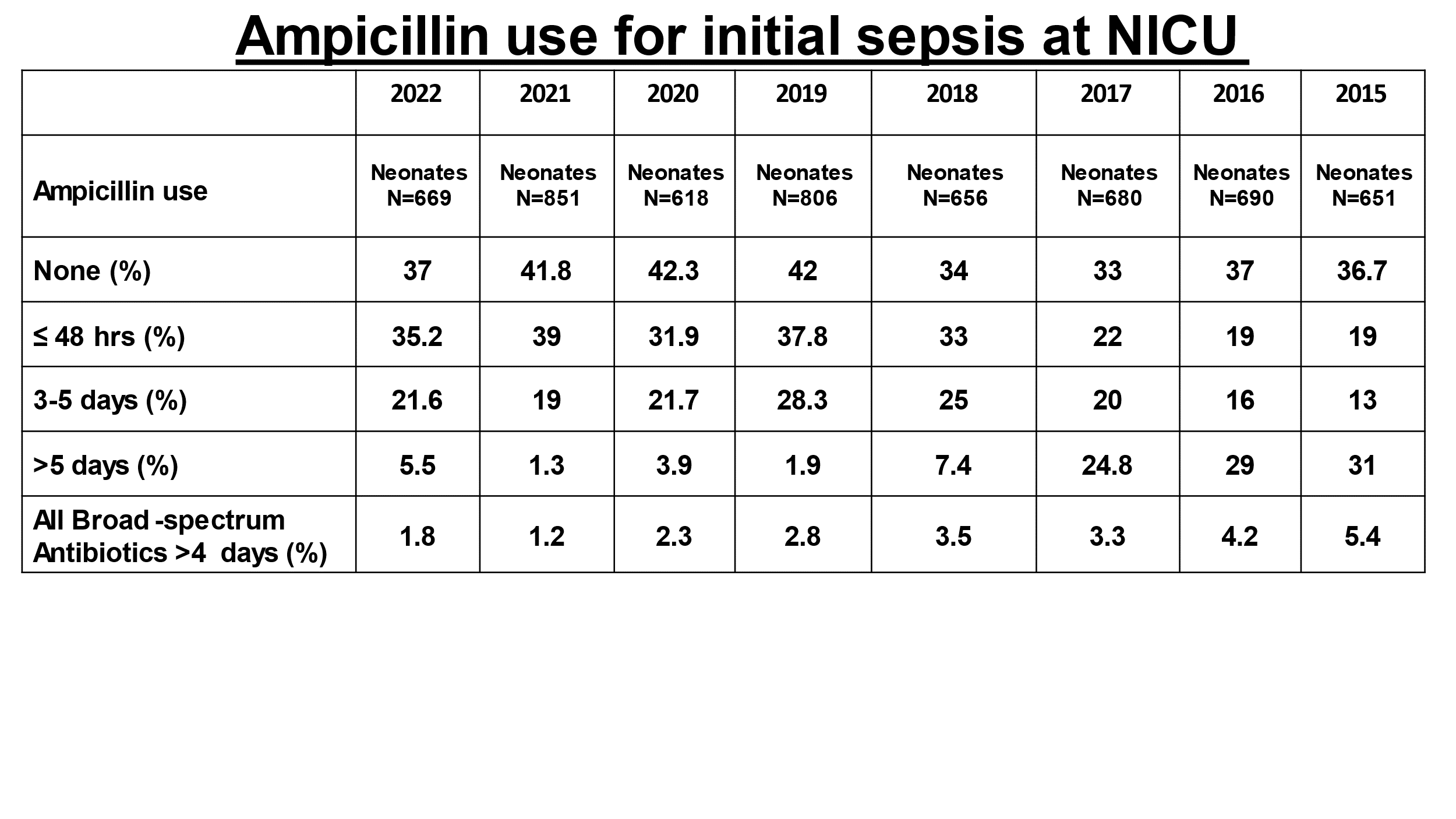
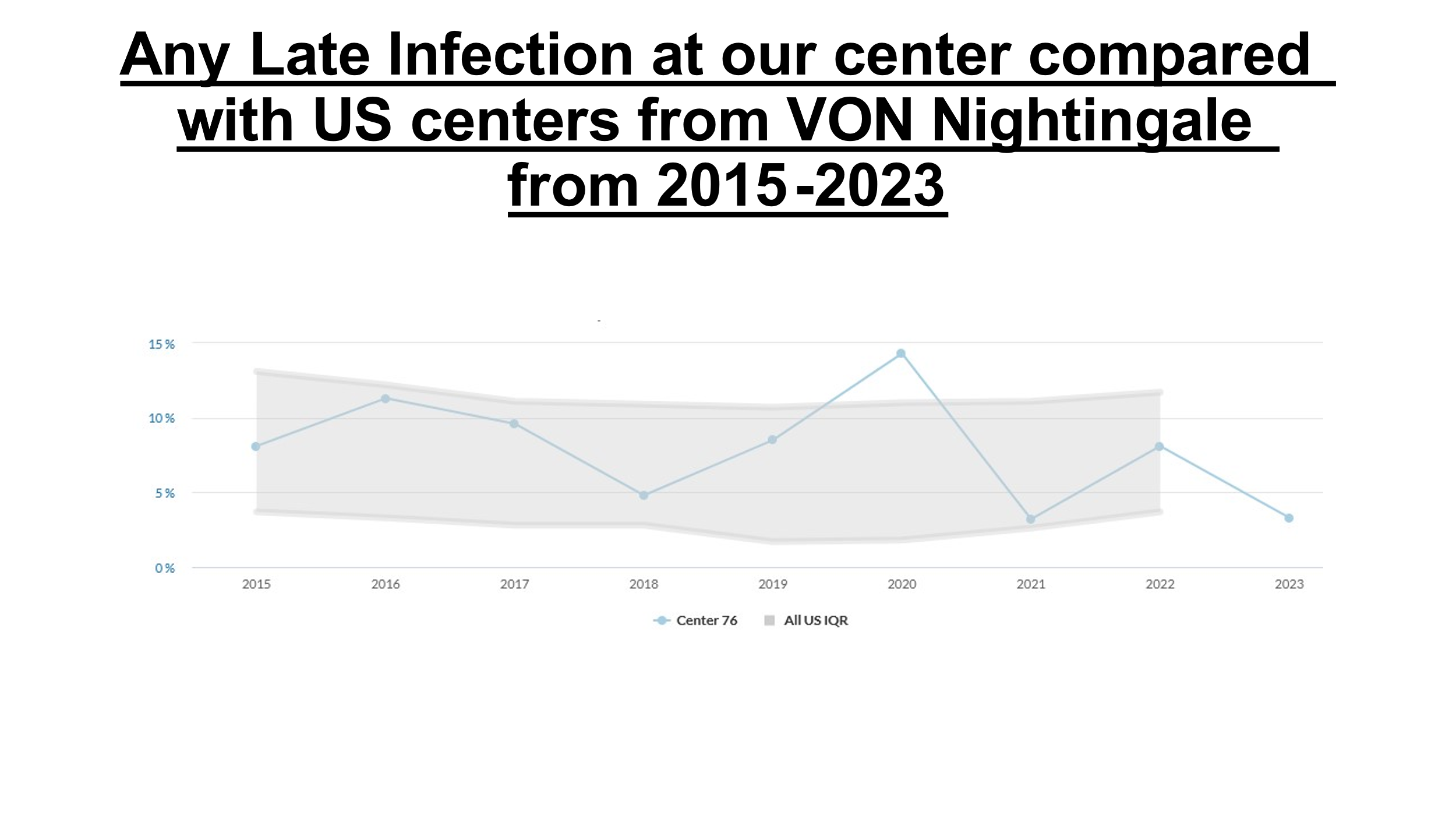
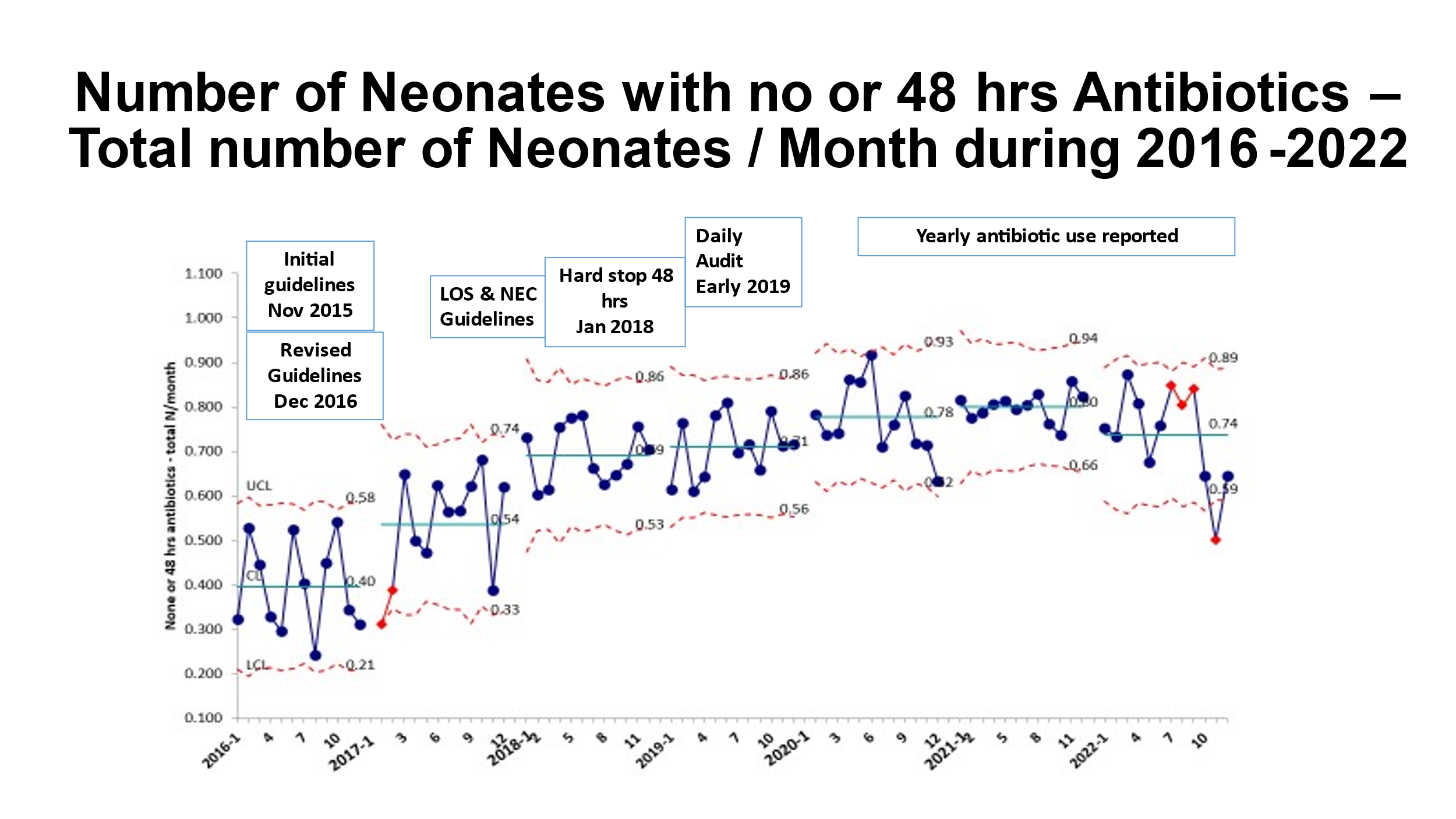
Background: Antibiotic over-use remains to be a major concern across many NICUs resulting in increased risk of neonatal morbidities. Implementation of NICU-specific antibiotic Stewardship through quality improvement project has been demonstrated consistently improved antibiotic prescription by practitioners and improve clinical outcomes Objective: To evaluate the overall antibiotic utilization and prescription practice at a level 3 Regional Neonatal Intensive Care Unit (RNICU) over 7 years after implementation of Antibiotic stewardship Design/Methods: A Quality Improvement (QI) project was planned and designed along with the pediatric Infectious disease physician initially by creating guidelines with antibiotics algorithms for early onset sepsis for < 35 weeks and >35 weeks neonates in 2016. After initial education to the medical team, antibiotic use data was presented regularly to the medical team as a part of the PDSA cycle and as the next step, an EMR hard stop at 48 hours was initiated in 2018. We are presenting Ampicillin use as marker of antibiotic use for early onset sepsis. The EMR data was collected from 2015 to 2022 and was analyzed using QI Macro for Excel statistics Results: The implementation of antibiotics algorithms have shown a consistent and progressive decrease in length of antibiotic use from 2018 onwards (table-1). Initiation of hard stop at 48 hours with negative blood cultures decreased neonates receiving longer antibiotics and improved compliance of 5 days antibiotics for clinical sepsis / Pneumonia without restart of antibiotics or increased use of broad-spectrum antibiotic. Any nosocomial Late onset Infection remained stable and decreasing ( Fig-1). A p - control chart shows the interventions and no or < 48 hrs antibiotics usage in neonates admitted to NICU has increased over the period from 0.4 to 0.74 mean (Fig-2)
Conclusion(s): We have observed that with consistent use of guidelines and regular education and reporting antibiotic use data, the duration of antibiotic use can be limited and can be sustained. As the next step, we plan to decrease antibiotics to 36 hours with negative blood culture in all neonatal populations

 photo")