Fellow University of Michigan Ann Arbor, Michigan, United States
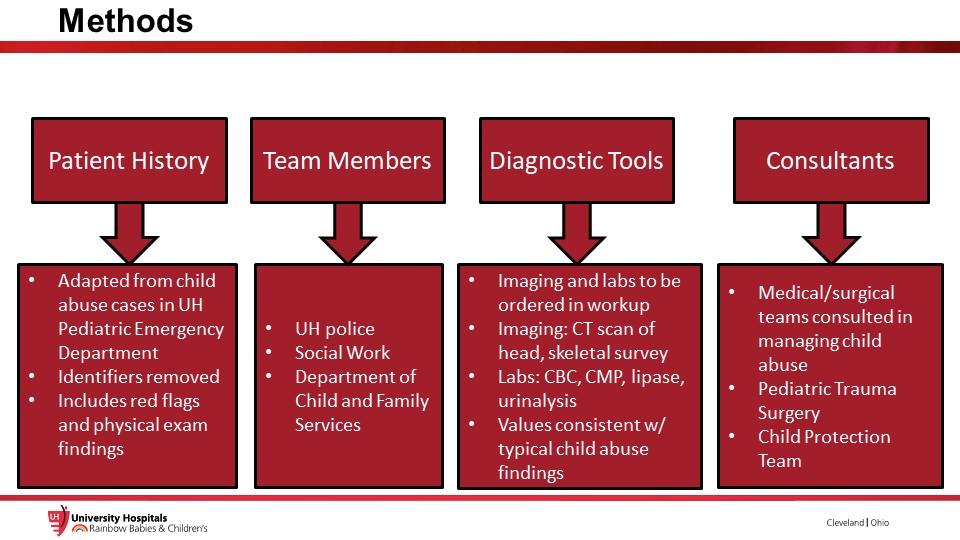
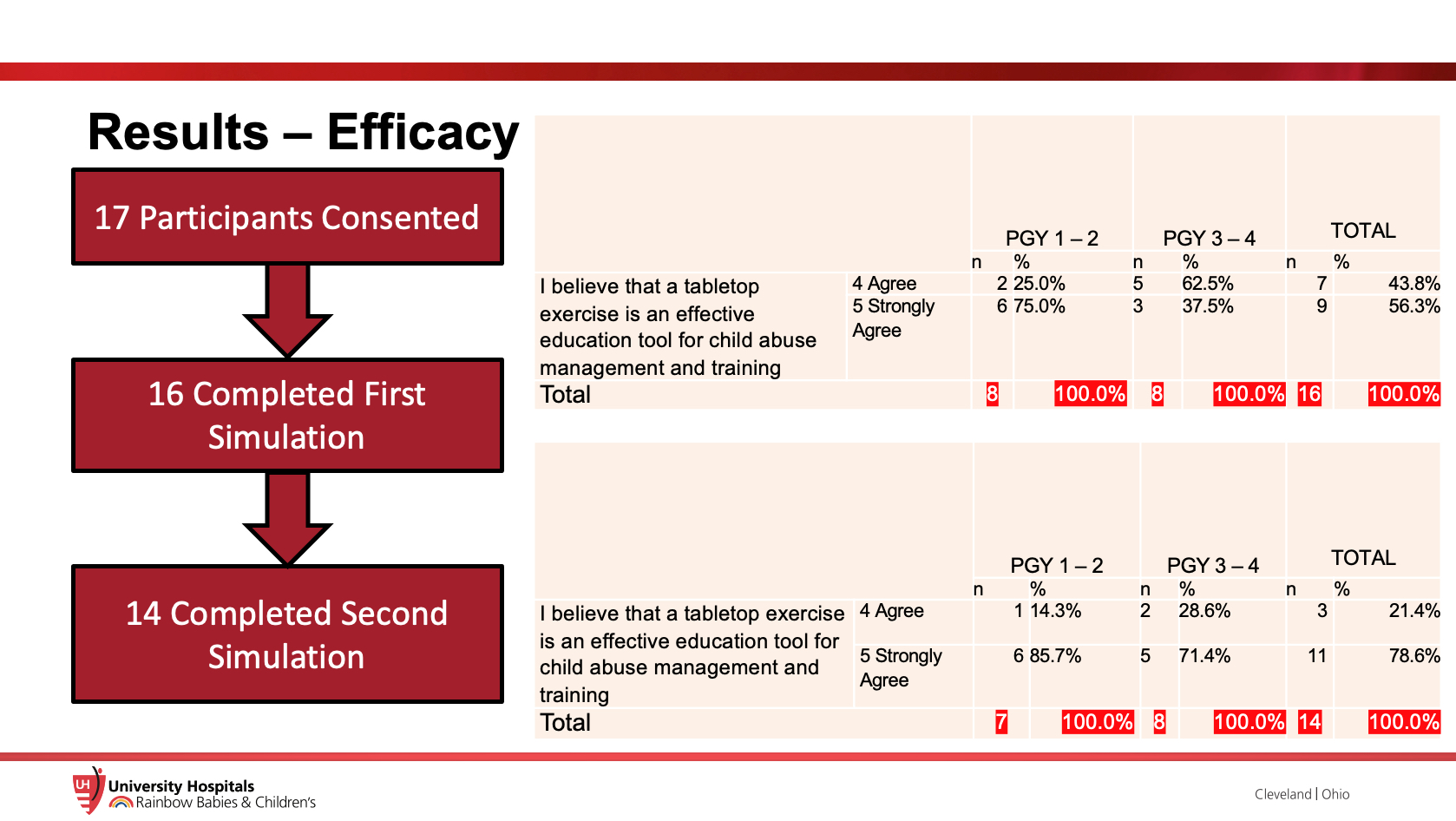
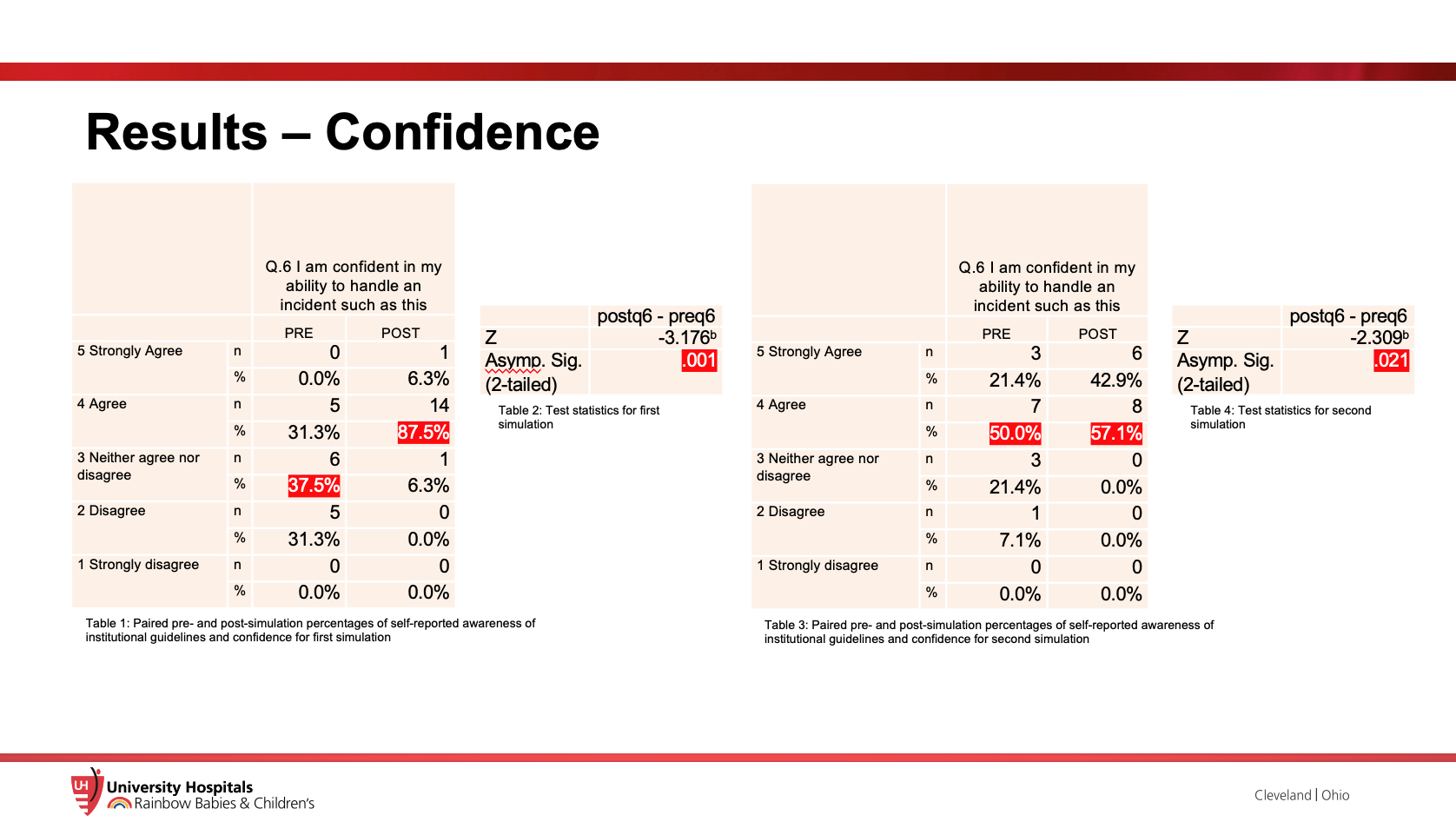
Background: The identification and management of child abuse victims is a foundational skill that all pediatricians must master. While studies demonstrate ongoing need for improved education, few validated curricula or clinical exercises exist. To address this deficit, a pilot study was conducted to assess the feasibility of using tabletop simulations to improve pediatric residents’ knowledge and confidence in managing pediatric physical abuse patients. Objective: To assess the feasibility of using tabletop simulations to improve pediatric residents’ knowledge and confidence in managing pediatric physical abuse patients. Design/Methods: Pediatric and internal medicine-pediatric residents completed tabletop simulations involving management of a child abuse patient in the pediatric emergency room. The simulation was conducted with a preceptor providing flashcards with case details to residents. Residents obtained each flashcard by asking pertinent questions related to history and exam, and subsequently making decisions about patient workup and disposition. Two simulation sessions were presented three months apart. Residents’ knowledge and confidence were assessed with pre and post surveys at each simulation. The surveys consisted of 3 multiple-choice knowledge-based questions, while trainee confidence was assessed with 5 questions using a 5-point Likert scale. Statistical analysis was completed with Wilcox Signed Ranks Test. Results: 17 residents from pediatric and internal medicine-pediatric residents were recruited. 16 residents completed the first tabletop simulation; 14 residents completed the second tabletop simulation three months later. All the residents agreed that the tabletop exercise was an effective education tool. Resident knowledge about child abuse management increased immediately after each simulation (p values < 0.001, 0.003) while they did not demonstrate knowledge retention between simulations (p values 0.705, 0.102). Resident confidence in managing physical child abuse improved after each simulation (p values 0.001, 0.021).
Conclusion(s): This pilot study demonstrated that tabletop simulations are a low-cost, low-fidelity educational tool that improves resident knowledge and confidence in managing pediatric patients who suffer from physical abuse. Future research should assess how to prevent knowledge decay during the 3 months between simulations, the feasibility of conducting simulations in groups versus individuals and the efficacy of the simulation between pediatric and non-pediatric residents.

 photo")