Neonatology Fellow The Warren Alpert Medical School of Brown University Maine Medical Center Providence, Rhode Island, United States
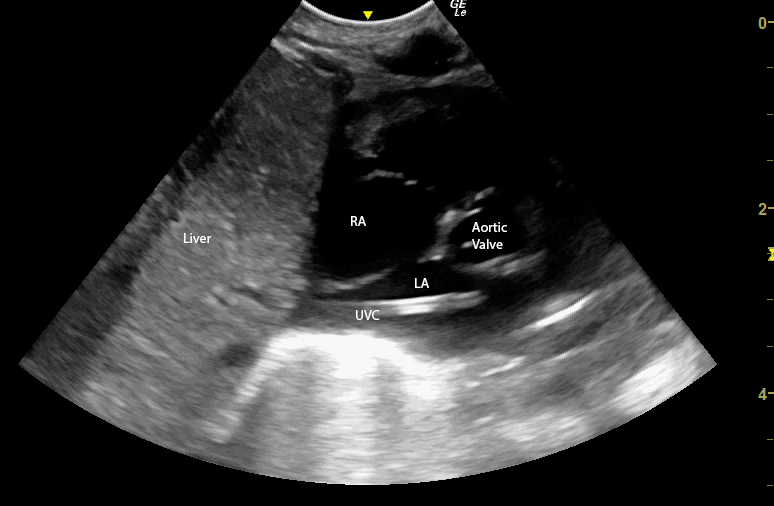
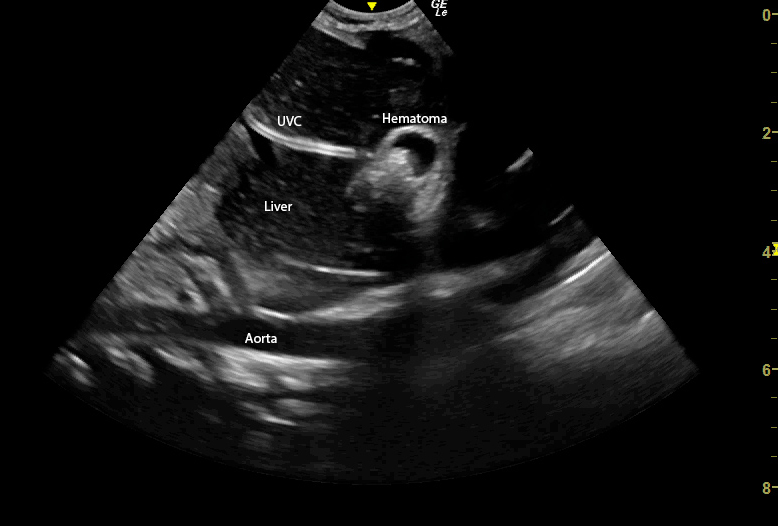
Background: X-ray is the standard of care to determine UVC position in most NICUs in the USA. However, point of care ultrasound (POCUS) can more accurately provide the exact anatomic location of the catheter tip. Whether x-ray can identify the true anatomic position of the line as shown by ultrasound has not been fully determined. Objective: To investigate whether x-ray can accurately identify correct UVC tip position. Design/Methods: This study involved neonates of any weight and gestational age admitted to the NICU who had a UVC placed. Data from infants who had an x-ray and ultrasound performed within the same 24-hour period were included. Anatomic location of the line by ultrasound was recorded as being in the ductus venosus (DV), cavoatrial junction, right atrium (RA) or left atrium (LA) using standard cardiac views. Line tip position on AP film was determined as per radiologist interpretation. Ultrasound and x-ray were then compared, and the anatomic location of the UVC on ultrasound was categorized as being either higher, lower or at the same anatomic location as the line on x-ray. The nonparametric sign test was used to compare anatomic position. Results: A total of 31 infants with 55 ultrasound/x-ray pairs were studied. The median gestational age and birth weight were 28.6 weeks and 1.1 kg, respectively. Agreement between x-ray and ultrasound was found in 39% of cases. When x-ray and ultrasound were not concordant, POCUS showed the UVC tip to be higher than it appeared on x-ray 85% of the time, and lower only 15% of the time (p < 0.0001). Interestingly, 27% of ultrasounds revealed the UVC to be in the LA (Image 1); none of these UVCs were identified as being in the LA on x-ray. Additionally, for lines identified as being at the cavoatrial junction on x-ray, 74% were found to in fact be intracardiac on ultrasound. Of note, one ultrasound in this study found a malpositioned UVC in the left portal vein with an associated TPN extravasation and hematoma (Image 2); unfortunately, x-ray interpretation of this line noted it to be at the cavoatrial junction, and failed to show that the line was malpositioned (Image 3).
Conclusion(s): Our data suggest that x-ray only identifies correct UVC position in just over one third of cases. When x-ray does not correctly recognize line tip position, POCUS most often reveals the UVC tip is higher than it appeared on AP film. Given the risks associated with malpositoned catheters, relying solely on x-ray to determine proper position of UVCs may be insufficient, and NICUs should be encouraged to develop programs to identify correct anatomic position of UVCs by ultrasound.

 photo")
.png)