Resident New York University Grossman School of Medicine New York, New York, United States
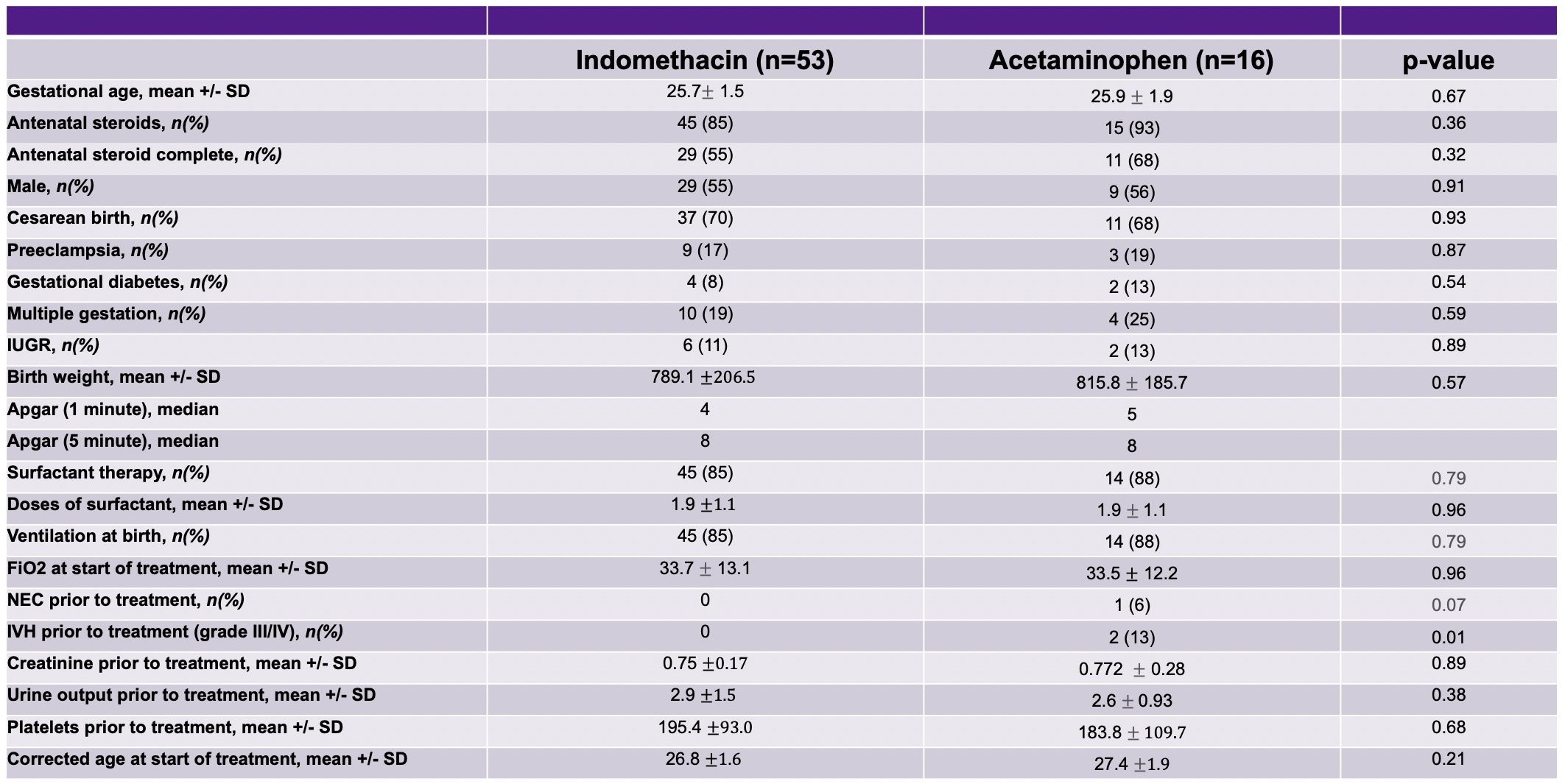
Background: A PDA can be treated with medication (indomethacin, ibuprofen, or acetaminophen) or directly via surgical ligation or a catheter-based method. In our neonatal intensive care unit (NICU), clinicians can either use indomethacin or acetaminophen as initial pharmacological treatment, followed by additional treatment(s) with medication as needed or via planned procedure. It remains unclear from prior studies which pharmacological treatment for PDA closure is best. Objective: To determine which medication, indomethacin or acetaminophen, was associated with the highest rate of PDA treatment success when used as initial pharmacological treatment. We also evaluated for any major differences in NICU course after treatment. Design/Methods: IRB approved retrospective chart review of inborn infants born < 30 weeks GA at NYULMC over a 5 year period (2017-2021). Subjects were placed into two cohorts: those who received initial treatment with indomethacin or initial treatment with acetaminophen. Treatment success was defined as post-treatment echo showing absent or small residual PDA only. We used a REDCap database to collect demographic and clinical data. Student T Test, Chi-Square Test, and Fisher Exact Test were utilized for analysis. Results: Overall, there was no difference in baseline characteristics between groups (Table 1) except for severe IVH at time of treatment initiation. We found that primary PDA closure success rates after initial medication trended higher in subjects who received indomethacin compared to acetaminophen (66.0% v. 43.8%, p=0.11). In subjects who received indomethacin first, we saw a trend towards needing less additional medication for closure (Figure 1) and less need for PDA ligation or interventional closure (15.1% v. 31.3%, p=0.27). Regarding NICU course, there was no difference in mortality, 7.5% v. 6.3%, p=0.86 or other major morbidities (Table 2).
Conclusion(s): We did not find a statistically significant difference in PDA closure rate after initial treatment with indomethacin compared to acetaminophen. However, there was a strong trend towards higher PDA closure success rate and less need for non-medication intervention in the indomethacin group. There does not appear to be a difference in NICU morbidity or mortality when comparing treatments. This study may have been limited by sample size, as it was a single-site study. We plan to expand the period studied to include more subjects to increase the power. Further studies are needed to evaluate initial medication effectiveness and assess for long-term neurodevelopmental impact of the initial medication.

 photo")
.jpg)
.jpg)