Chief Scientist, Patient Monitoring Medtronic Edinburgh, Scotland, United Kingdom
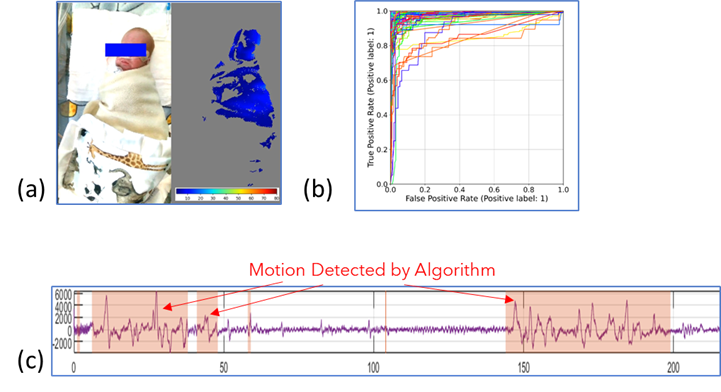
Background: The degree of neonatal activity, which we define here as gross body movements of the torso, head or limbs, may vary with physiologic state, level of sedation or underlying pathology. Neonatal activity is also the cause low frequency motion noise in physiological signals, which may lead to false or failed readings of parameters including heart rate or respiratory rate. It is imperative to monitor vital signs reliably as management decisions are made based on these parameters. In addition, attaching probes to monitor vital signs may damage the skin of premature infants. Objective: These considerations prompted the development of a novel neonatal activity monitoring technology using a machine learning algorithm trained on features extracted from the video stream of a commercially available depth sensing camera (Intel RealSenseTM D415). This non-contact, or touchless, technology allows continuous monitoring without attaching probes to the neonate. Here we report the preliminary results of the model using data from two neonatal intensive care units. Design/Methods: For this proof-of-principle study, data captures from 20 neonates (10 from each site) were assessed. These comprised of depth information acquired from up to six camera locations above and to the side of each neonate. Test videos were analyzed in which only the neonate was present in the scene, for a total of 84 videos. Data were manually labelled for neonatal motion using an RGB video stream collected synchronously with the depth data. Each depth dataset was processed to provide a range of input features based on depth changes corresponding to neonatal activity. Figure 1a shows an example of a neonate with the associated depth changes over a 1 second epoch. The derived features were input into a random forest machine learning model. Training and testing employed a leave-one-subject-out cross validation paradigm which provides an indication of the model stability. Results: The calculated Receiver Operator Curves (ROC) are shown in Figure 1b. The mean [standard deviation] of the sensitivity and specificity of the optimal points and the corresponding area under ROC (AUROC) were 93.0% [10.0%], 92.0% [13.7%] and 97.8% [3.6%], respectively. The activity identified by manual labelling matched well with the noisy segments on the corresponding respiratory flow signal. An example of a flow waveform with identified motion is shown in Figure 1c.
Conclusion(s): Our findings indicate the viability of non-contact, continuous, neonatal activity monitoring using a depth sensing camera. Future work will aim to perform blind testing of larger datasets.