Neonatology Fellow University of Mississippi School of Medicine Jackson, Mississippi, United States
Background: Thoracentesis is an emergency lifesaving procedure for pneumothorax. Neonatal Resuscitation Program (NRP) recommends using either the mid-clavicular line (MCL) or anterior-axillary line (AAL). However, there is no recommendation for the depth of needle insertion in either preterm or term infants. Improper needle placement during thoracentesis may cause damage to vital structures or death. Adult studies have shown that AAL is the optimal site for thoracentesis as MCL may be dangerously close to vital structures. There are no studies in preterm or term infants to determine the safe site for thoracentesis. Objective:
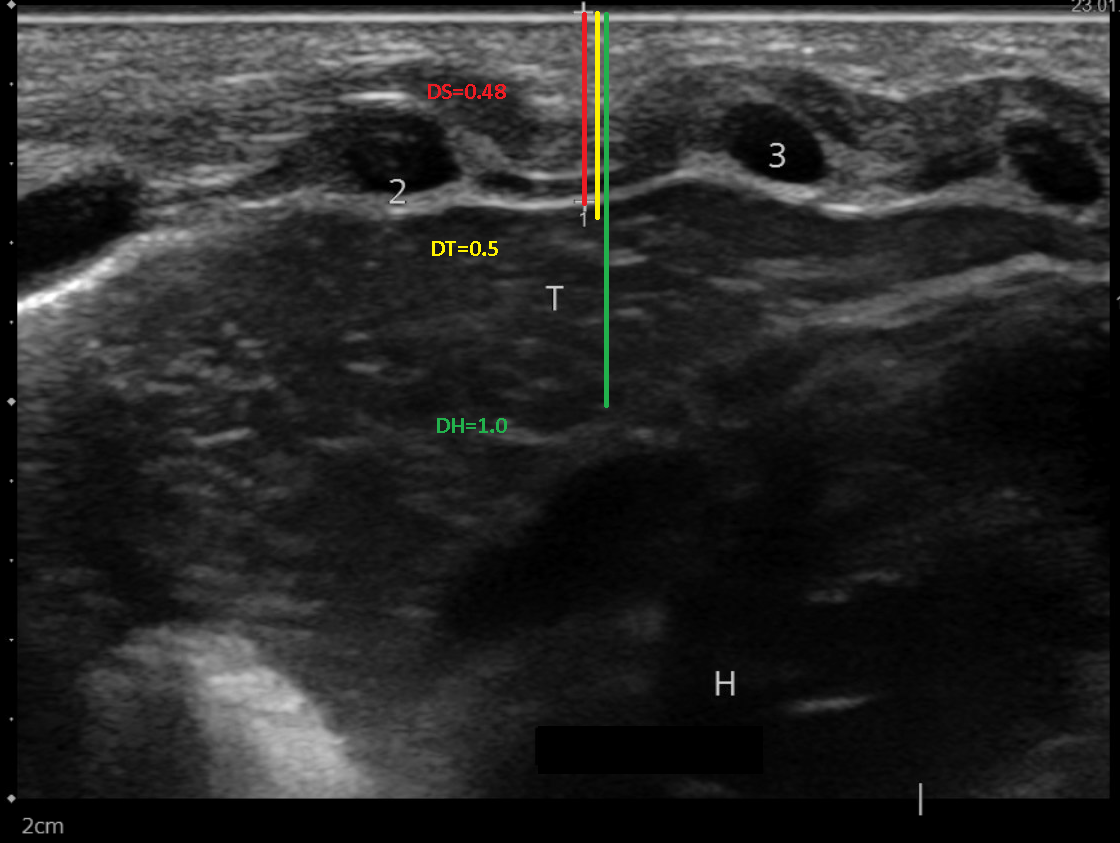
Aims: 1) to determine the distance between the skin and the pleural space (DS) at MCL and AAL in preterm and term infants. 2) To determine the frequency of vital structures at each site for thoracentesis. Design/Methods: From July 2022 to August 2023, this prospective study enrolled sixty-two neonates born at the University of Mississippi Medical Center (UMMC) with gestational ages (GA) from 23-41 weeks. Those with pneumothorax, chest wall anomalies, or malpositioned great vessels were excluded. We used a high-frequency ultrasound (US) linear probe (9MHz) to determine the DS in participants at the right and left MCL (2nd intercostal space) and AAL (4th intercostal space), respectively, as recommended by NRP. The Pediatric Radiologist measured the DS. These measurements were analyzed with GA, birth weight (BW), sex, and race. Vital organs (VS): considered significant when seen within the US window and 2cm from the insertion site (Figure 1). Results: About 56.5% of the infants were male. The mean GA was 32w2d (23-41 weeks). Mean BW- 1851.61 g and the range 400-4815 g. The mean DS at left MCL, right MCL, right AAL, and left AAL were 0.54 cms, 0.53 cms, 0.54 cms, and 0.53 cms, respectively. The DS increased linearly from 23 weeks to 41 of GA (p= < 0.0001) (Table). No correlation was, however, noted between sex, race, and DS. VS were most commonly seen at left MCL (48.4%), followed by 3.2% at right MCL, 1.6% at left AAL, and 0% at right AAL, respectively. The relationship between GA, DS, and depth of VS at the left MCL are shown in Figure 2.
Conclusion(s): We have determined the appropriate depth for the safe insertion of a thoracentesis needle in infants between 23 and 41 weeks of gestation. Our findings contradict the common practice, as we discovered that the heart and thymus are often situated very close to the MCL sites, especially on the left side. We, therefore, recommend using the AAL site for thoracentesis in newborns of any gestational age, as it is the safest option available.

 photo")

.png)