Student University of Waterloo Waterloo, Ontario, Canada
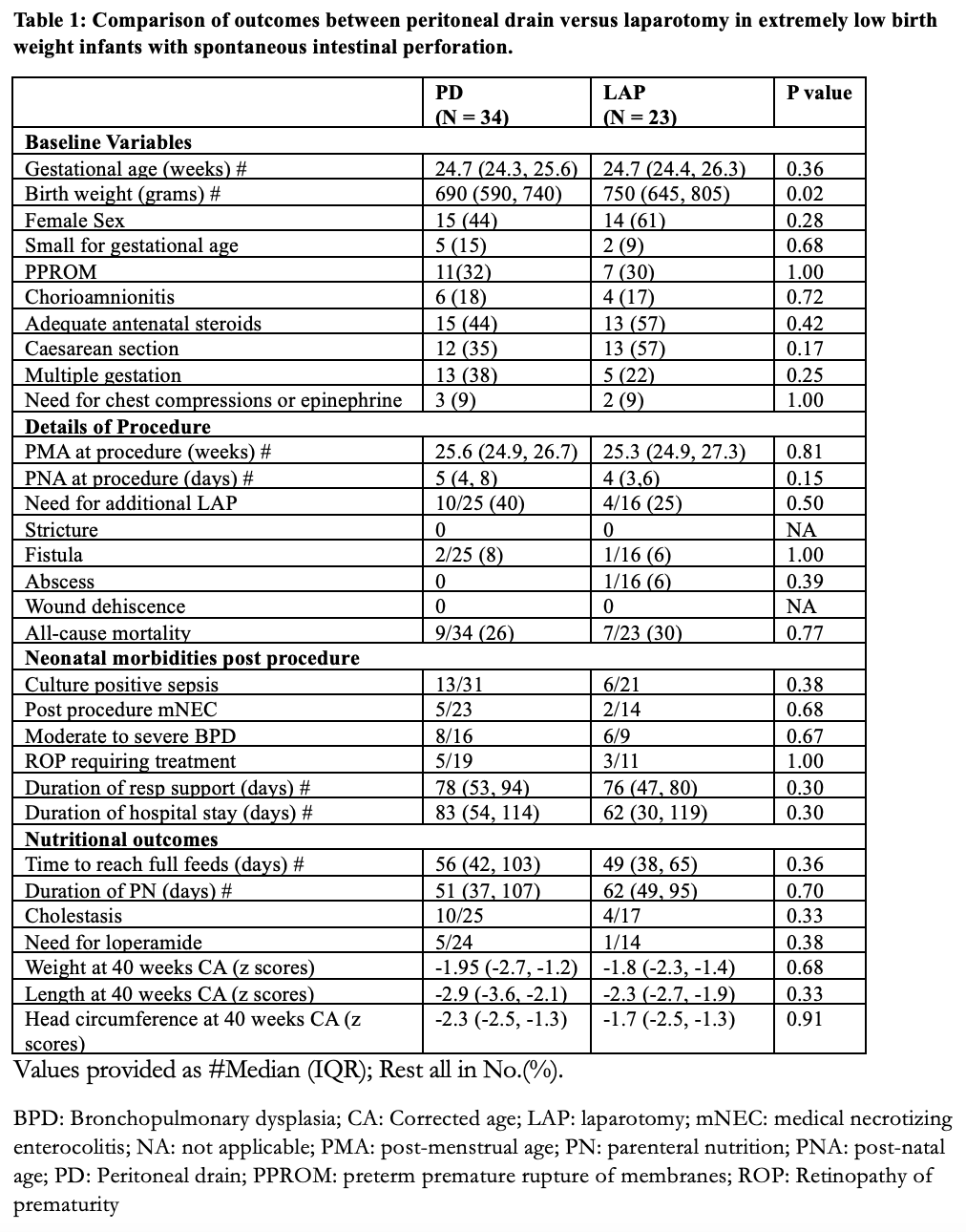
Background: The two common approaches for surgical management of spontaneous intestinal perforation (SIP) in preterm neonates are peritoneal drain (PD) insertion that can be done at the bedside under local anesthesia and exploratory laparotomy (LAP) though definitive may be associated with short term complications related to procedure and general anesthesia. There is no consensus due to limited literature available regarding the optimal surgical approach in extremely low birth weight (ELBW: birth weight < 1000 grams) neonates with SIP. Objective: To compare short- term outcomes of PD versus LAP as initial surgical modality in ELBW infants with SIP. Design/Methods: We conducted a retrospective cohort study of ELBW infants with SIP at a single quaternary neonatal intensive care unit between January 1, 2013, and December 31, 2022, who underwent first intention PD or LAP. The pre-specified outcomes included need for additional laparotomy, post-procedural complications, rates of cholestasis, medical NEC, pre-discharge mortality, nutritional outcomes, neonatal morbidities and anthropometric indices (weight, length, head circumference z-scores) at 40 weeks postmenstrual age or discharge. Mann-Whitney U test and Fisher’s exact test were used for comparing continuous and categorical data respectively between the two groups. Results: Of the 57 ELBW infants with SIP included, 34 (60%) infants underwent PD, and 23 (40%) infants underwent LAP. The baseline characteristics, details of procedure including complications, neonatal morbidities and nutritional outcomes are outlined in Table 1. Compared to the LAP group, the infants in the PD group were smaller (690 vs 750 g; p=0.02). There was no statistically significant difference in rates of need for additional laparotomy amongst the two groups [PD (40%) vs LAP (25%); p=0.50]. There was no significant difference between the two groups for other pre-specified procedural related complications, neonatal morbidities and nutritional outcomes.
Conclusion(s): Our local 10-year data from a high volume quaternary surgical centre suggests that both peritoneal drain and exploratory laparotomy are comparable with regards to short term outcomes in ELBW infants with SIP.

 photo")