Pediatric Resident Mount Sinai - Elmhurst Queens, New York, United States
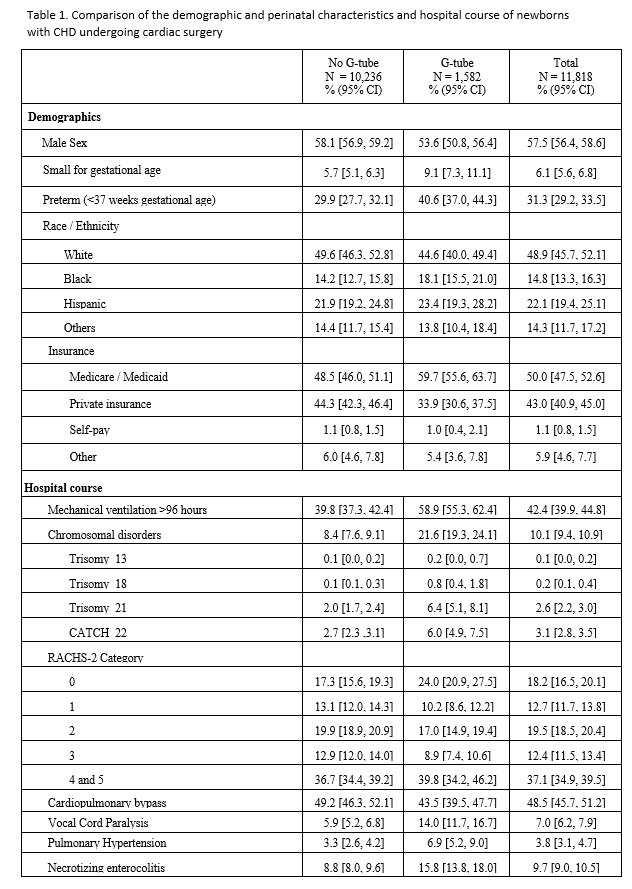
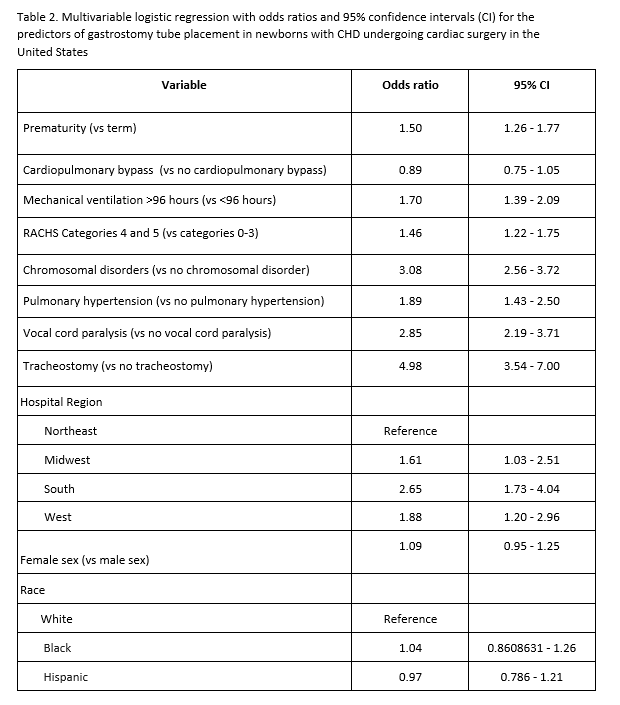
Background: Feeding difficulties and the need for gastrostomy tube placement (GT) in newborns with congenital heart defects (CHD) who undergo cardiac surgery are very common. Failure to achieve full oral feeding at discharge is associated with neurodevelopmental delays and the identification of risk factors associated with this can help to devise strategies that improve the outcomes for these infants. However, the few studies that have examined these risk factors are single-center studies with small sample sizes and mixed results. Objective: To identify the prevalence and the factors associated with GT placement at discharge in newborns with CHD who underwent cardiac surgery during the birth hospitalization. Design/Methods: This was a retrospective, cross-sectional analysis of the 2016 and 2019 Kids Inpatient Database. Newborns (admission age < 28 days) with major CHD who had cardiac surgery (assigned a Risk Stratification for Congenital Heart Surgery) were identified with ICD-10 codes, and those who survived to discharge were dichotomized into those with and without GT. Infants with isolated cardiac defects (PDA, VSD, ASD) were excluded. The demographic and perinatal characteristics, and the hospital course were compared using Chi-square or Wilcoxon-Rank sum test, as appropriate. The exposure variable was CHD with cardiac surgery and the outcomes of interest were the prevalence and predictors of GT placement. A priori set of covariates and other clinically relevant variables were entered into a multivariable logistic regression analysis to identify the predictors of GT placement. Results: Among 7.724 million neonatal admissions, 38,053 had CHD (4.9/1000). Of these, 11,818 had RACHS-2 classification and were included in the study. The prevalence of GT was 13.3% (1,582/11,818). The characteristics of the study population are shown in Table 1. Compared to those without GT, those with GT were more likely to have Medicaid, be ventilated for >96 hours, be preterm, have chromosomal disorders, have vocal cord paralysis, pulmonary hypertension, and longer length of stay (89 vs 31 days) and higher hospital cost ($349,479 vs 172,847). In the adjusted analysis (Table 2), tracheostomy placement, prematurity, mechanical ventilation >96 hours, chromosomal disorders, pulmonary hypertension, RACHS-2 ≥4, and vocal cord paralysis. Cardiopulmonary bypass and sex were not associated with increased odds of GT placement.
Conclusion(s): These findings can be used for counseling families and the early identification of newborns who would require GT can potentially reduce length of stay and hospital cost.

 photo")