Medical Student UBC Faculty of Medicine Cawston, British Columbia, Canada
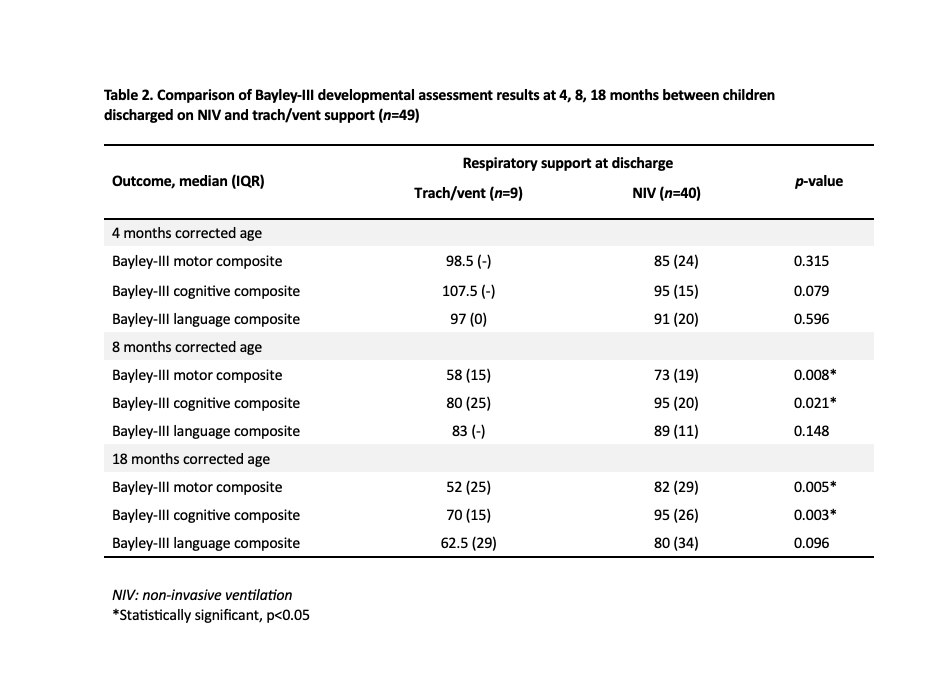
Background: Improved survival at increasingly low gestational ages (GA) has resulted in a growing population of infants with bronchopulmonary dysplasia (BPD). In cases of severe BPD, ongoing respiratory support may be needed after neonatal unit (NICU) discharge. Treatment options include low-flow oxygen (LFO2), non-invasive ventilation (NIV), and ventilation via tracheostomy (trach/vent). Objective: To characterize the population of infants with BPD who require respiratory support after NICU discharge, and describe trajectory including long-term clinical outcomes and differences in outcomes according to type of home respiratory support. Design/Methods: Retrospective study of infants ≤32 weeks GA with BPD and use of respiratory support at NICU discharge in British Columbia, 2013-2022. Cases were identified from hospital coding and provincial NICU follow-up and home ventilation patient databases. Serial growth and neurodevelopmental measures were collected at 4, 8, and 18 months corrected age, 3 and 4.5 years. Results: 102 infants with BPD (66% male, 22% multiple birth) were discharged on home respiratory support. Median GA was 25 weeks and birthweight 727g. Home support was with trach/vent in 9% (n=9), NIV in 39% (n=40), and LFO2 in 52% (n=53). Median corrected age at tracheostomy insertion was 3.8 months. Characteristics of children in NIV and trach/vent groups were similar, apart from a higher prevalence of medically managed pulmonary hypertension and older age at successful extubation in the trach/vent group (Table 1). Infants with trach/vent were older at NICU discharge (median 391 vs 210 days, p< 0.001) and stopping ventilation (median 4.6 vs 1.7 years, p< 0.001) than those discharged on NIV. In LFO2 treated children, median age at stopping O2 was 9 months. Bayley-III scale cognitive and motor composite scores were similar in infants supported with NIV and trach/vent at 4 months, but significantly lower in the trach/vent group at 8 and 18 months (Table 2). There was no difference in median weight-for-age z-scores between the two groups at any time point. Hospital readmission within 2 years of NICU discharge was more common in infants with trach/vent than NIV (89% vs 62%). All children were alive at median 4.5 years follow-up.
Conclusion(s): Use of home NIV to support infants with BPD is associated with shorter NICU admission and ventilation duration than trach/vent. No advantages of trach/vent over NIV were identified in terms of neurodevelopment or growth. These findings endorse use of home NIV in infants with BPD assuming they are not fully ventilator dependent.

 photo")
.jpg)