Fellow Ann & Robert H. Lurie Children's Hospital of Chicago Atlantic Health System Inc Chicago, Illinois, United States
Background: Hypoxic ischemic encephalopathy (HIE) is a common cause of mortality and severe disability. HIE is diagnosed with a combination of biochemical and clinical findings. Neonates with moderate to severe HIE benefit from therapeutic hypothermia (TH) starting within 6 hours of life. Earlier than 3 hours of life gives optimal neuroprotection, hence prompt diagnosis of HIE is preferable.
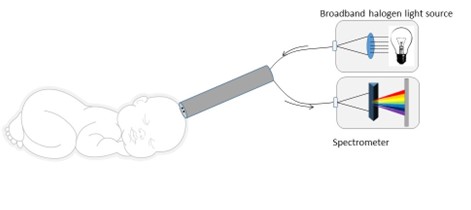
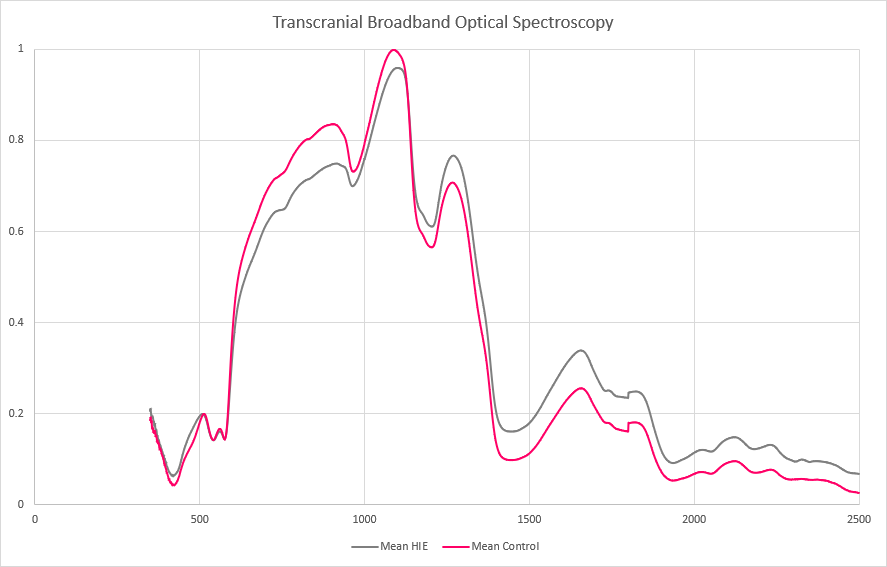
Broadband optical spectroscopy (BOS) uses a noninvasive infrared reflectance light measurement, consisting of a handheld probe connected to a broadband halogen light source via fiberoptic cables, coupled with a spectroradiometer that detects a wide range of wavelengths (Figure 1). BOS offers 500 times greater granularity than commercially available near-infrared oximeters. BOS involves contact with the skin for less than a second and does not generate warmth or discomfort and avoids exposure to ultraviolet rays or ionizing radiation. BOS may improve the early diagnosis of neonates that may benefit from TH. Objective: To demonstrate areas of maximal differences in spectroscopy signals in neonates with HIE, compared to healthy controls. Design/Methods: Neonates were identified as candidates for TH on admission to the NICU, and healthy controls underwent transfontanellar BOS. Controls were age-matched neonates without critical illness or intracranial pathology. Inclusion criteria consisted of neonates >/= 36 weeks gestational age (GA) with moderate to severe HIE, eligible for TH. Exclusion criteria were neonates < 36 weeks GA, birth weight < 1800g, and suspected subgaleal hemorrhage. Results: BOS was obtained from 12 neonates within the first 24 hours of life. There were 6 neonates with HIE eligible for TH, and 6 healthy controls; the median GA was 39.4 weeks and the median weight was 3.5 kg. No safety concerns or changes to clinical care were noted. Average spectroscopy signatures are shown in Figure 2. There were differences between the near-infrared and short-wave infrared portions of the curves.
Conclusion(s): Our pilot study presents differences in BOS data in neonates with HIE vs. healthy controls. This safe, non-invasive diagnostic tool may help early HIE detection and monitoring of at-risk neonates in the NICU. These findings suggest that BOS could be an adjunct to current clinical practices for HIE assessment in neonates, improving the identification of neonates eligible for TH and potentially other neuroprotective interventions.

 photo")