272 - Randomized trial of effectiveness and pharmacokinetics of 0.02 and 0.03 mg/kg doses of epinephrine via umbilical venous vs. peripheral venous routes in ovine perinatal cardiac arrest.
Trainee University of California, Davis Davis, California, United States
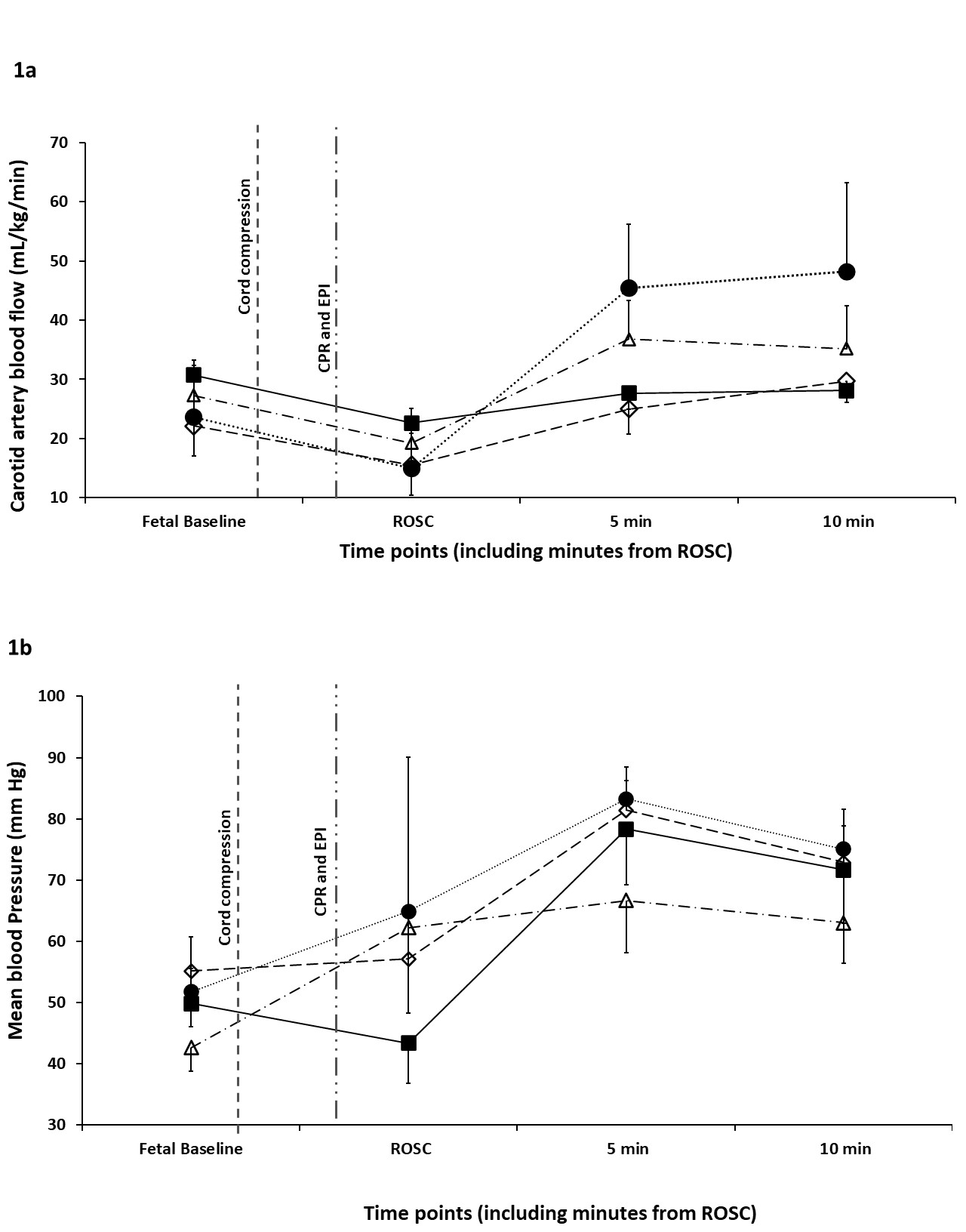
Background: Current guidelines recommend epinephrine (EPI) administration via a low-lying umbilical venous catheter (UVC) in neonatal cardiac arrest or bradycardia not responding to effective ventilation and chest compressions. However, UVC placement can take 5.4 ± 2.2 min (Halling et al 2017) and requires expertise and specialized equipment that may be a challenge for pre-hospital and non-neonatal providers. The 8th Edition of Textbook of Neonatal Resuscitation suggests 0.02 mg/kg as the initial dose of EPI but there are no randomized blinded trials comparing pharmacokinetics with 0.03 mg/kg. We hypothesized that a higher dose (0.03 mg/kg) of peripheral intravenous (PIV) EPI is as effective and will achieve similar plasma levels as 0.02 mg/kg of UVC EPI during neonatal resuscitation. Objective: Compare the incidence of return of spontaneous circulation (ROSC), time to ROSC, and plasma EPI concentrations between UVC and PIV routes using 0.02 and 0.03 mg/kg EPI during ovine perinatal asphyxial arrest. Design/Methods: Term fetal lambs were intubated and instrumented. Asphyxia was induced by cord occlusion until cardiac arrest. Following resuscitation with ventilation and chest compressions, lambs were randomized to one of 4 groups: UVC-0.02 mg/kg EPI, UVC-0.03 mg/kg EPI, PIV- 0.02 mg/kg EPI and PIV-0.03 mg/kg EPI followed by 3mL saline flush. Hemodynamics and plasma EPI concentrations were monitored. Results: Gestational age and birth weight were similar between the study groups (table 1). All lambs achieved ROSC with the first dose of EPI in the UVC and 0.02mg/kg PIV groups. One lamb in the PIV-0.03 mg/kg EPI did not achieve ROSC despite 4 doses of EPI. Among lambs that achieved ROSC, time to achieve ROSC was not different between groups (table 1). Carotid blood flow and mean blood pressures were similar at ROSC and after ROSC (figure 1a and 1b). Plasma EPI concentration was not different between 0.02 vs 0.03 mg/kg doses and UVC vs PIV routes (table 2).
Conclusion(s): Incidence of and time to ROSC and plasma EPI concentrations were similar between PIV and UVC routes using 0.02 mg/kg and 0.03 mg/kg doses of EPI, supporting the current NRP suggested initial EPI dose of 0.02 mg/kg. Further studies are warranted to study the feasibility, timing, and effectiveness of PIV route of EPI in newborns not responding to chest compressions. This simple technique may benefit newborns globally especially during resuscitation by pre-hospital and non-neonatal providers lacking expertise in UVC placement or in low resource settings without access to UVC equipment.

 photo")
.jpg)
.jpg)