pediatrician Stavanger University Hospital Hundvaag, Rogaland, Norway
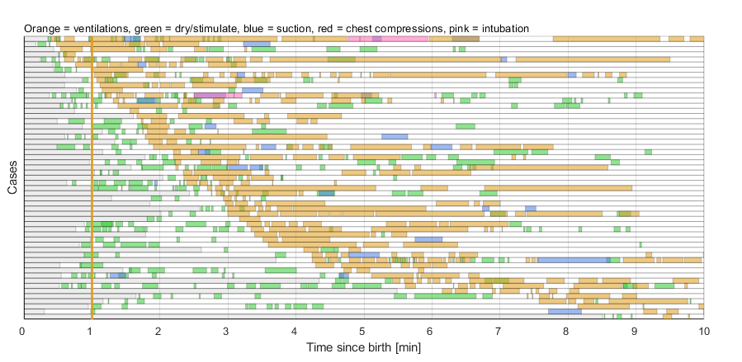
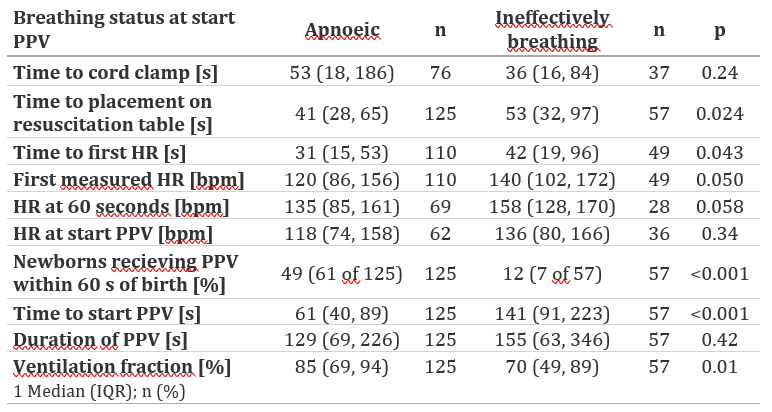
Background: Ventilation is considered the single most important step in newborn resuscitation. Between 3-10% of newborns fail to initiate spontaneous breathing and receive positive pressure ventilation (PPV) at birth. Initiation of PPV is time-critical and the risk of mortality and morbidity rises with prolonged apnoea. Newborn resuscitation algorithms and guidelines are focused on the sequence, timing and duration of interventions. Although clinical research has accelerated over recent decades, data collection is often incomplete and inaccurate. Automated capture, storage, and synchronisation of objective data offers promise of higher quality research and ultimately better methods of newborn resuscitation. Objective: To evaluate the use of newborn resuscitation timelines to assess and visualise the incidence, sequence, timing, duration of and response to resuscitative interventions. Design/Methods: A population–based observational study conducted June 2019 – November 2021 at Stavanger University Hospital, Norway. Parents consented to participation antenatally. Newborns ≥28 weeks’ gestation receiving PPV at birth were enrolled. Time of birth was registered. Dry-electrode ECG was applied as soon as possible after birth and used to measure heart rate continuously during resuscitation. Newborn resuscitation timelines were generated from analysis of video recordings. Results: Of 7466 newborns ≥28 weeks’ gestation, 289 (3.9%) received PPV. Of these, 182 had the resuscitation captured on video, and were included. Two-thirds were apnoeic, and one-third were breathing ineffectively at the commencement of PPV. The median (quartiles) birth weight and gestational age were 3584 g (2960-3984) and 40 weeks (38-41) in the apnoeic group, and 3358 g (2954, 3680) and 39 weeks (38,40) in the ineffectively breathing group. PPV was started at median (quartiles) 72 (44, 141) seconds after birth and continued for 135 (68, 236) seconds. The ventilation fraction, defined as the proportion of time from first to last inflation during which PPV was provided, was 85%. Interruption in ventilation was most frequently caused by mask repositioning and auscultation. PPV was commenced within 60 seconds of birth in 49% of apnoeic and 12% of ineffectively breathing newborns, respectively. Suctioning was performed in 35% of newborns, in 95% of cases after the initiation of PPV.
Conclusion(s): Newborn resuscitation timelines can graphically present accurate, time-sensitive and complex data from resuscitations synchronised in time. Timelines can be used to enhance understanding of resuscitation events in data-guided quality improvement initiatives.

.png)