9 - Amplitude integrated electroencephalography during retrieval of neonates at risk of hypoxic-ischaemic encephalopathy: a feasibility study in road and fixed-wing air transport in Western Australia.
Child and Adolescent Health Sevice Perth, Western Australia, Australia
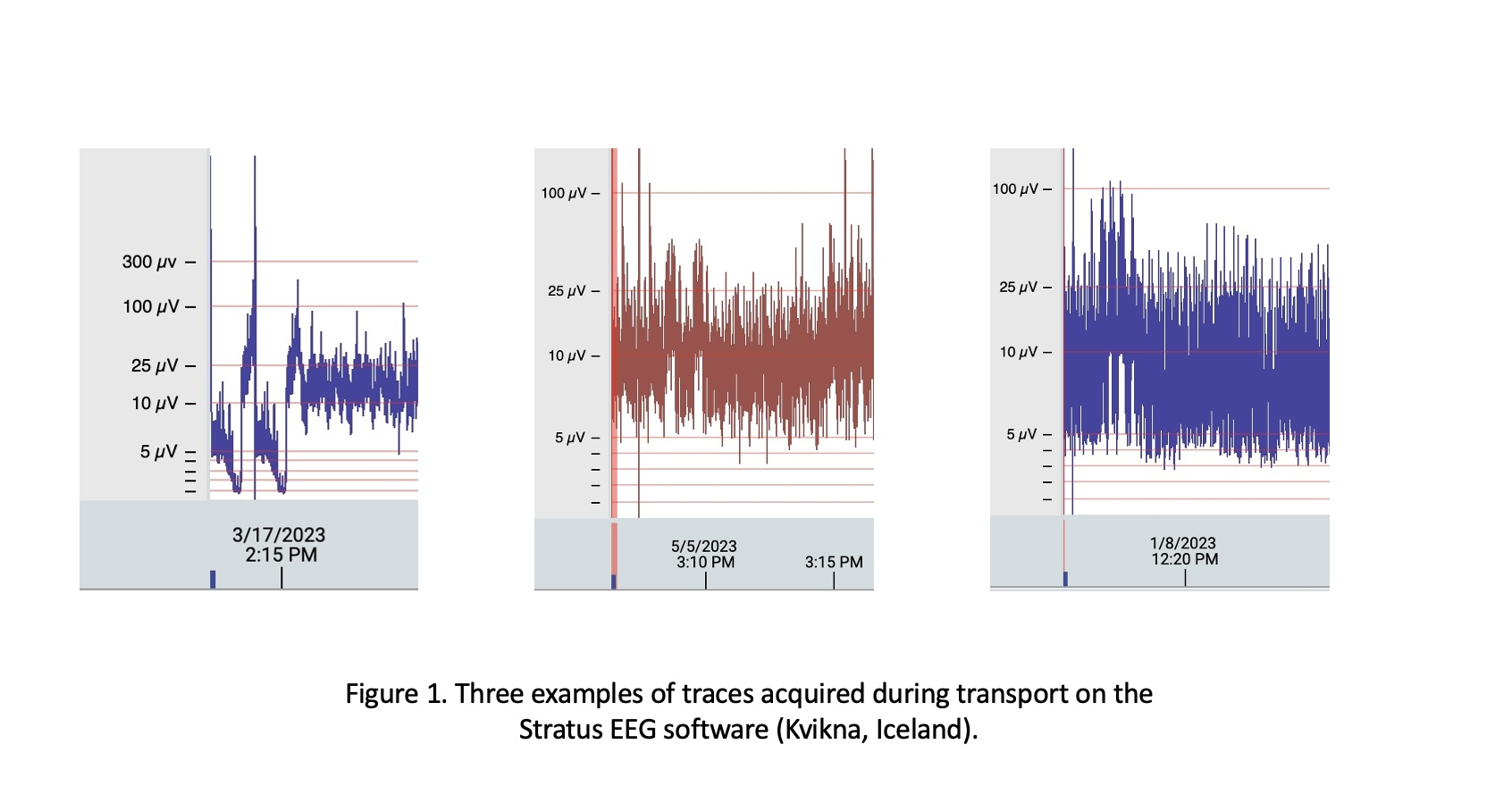
Background: Infants at risk of hypoxic-ischaemic encephalopathy require early identification and initiation of therapeutic hypothermia. Amplitude-integrated EEG (aEEG) is limited to tertiary centres in Australia and delayed if travel is necessary for definite care. Western Australia's (WA) area is 2.6 million Km2. There is no data on quality and reliability of aEEG during neonatal transport. Objective: We aimed to investigate whether portable aEEG can capture readable and accurate data during neonatal retrieval in WA. Design/Methods: All infants ≥ 35 weeks, at risk of HIE at referral, were eligible. Consent was obtained after arrival by the transport team. Low-impedance needle scalp electrodes (Natus Medical USA) were placed at C3/4 and P3/4 positions along with grounding, connected to an amplifier (Trackit T4, Lifelines Neuro, UK) and tablet computer with EEG software (Stratus EEG, Kvikna, Iceland). Readability was assessed as:1) Total artefact: Data reviewed independently by 3 experts with experience in neonatal aEEG. All were blinded to clinical outcomes. Traces were split into 15-min (approx.) segments. Each was read as artefact if >2 experts agreed. 2) Proportion of movement artefact: Trend aEEG was extracted from C3/4, and total time trace %>100 µV calculated. 3) No. of impedance (Z) alarms (>10KΩ) during each trace and their magnitude. Infants transported by air vs road were also compared by % movement artefact.
Demographic, transport and aEEG descriptives were recorded and presented using median (interquartile range (IQR). Total artefact expressed as % of total trace; movement artefact as mean (standard deviation (SD)) % time >100 µV of total trace; Z as mean no. (range) and magnitude as median (IQR). The recording was defined successful if >80% of all traces were total/movement artefact-free and low impendence. Student's t-test compared air vs road movement artefact. Results: During the study period (Sept ‘22 –June '23), 20 infants at risk of HIE were enrolled. In total, 38 hours of aEEG were recorded in neonatal transport. Transport aEEG extracts are shown in Fig 1. Table 1 contains population, transport and basic aEEG descriptives. No artefact was scored in 160/178 (89.9%) segments. aEEG trend >100µV for 244s (0.2%) of total recording. There were Z notifications in 4/20(20%) traces, mean 4(1 – 6); magnitude was 99.1(16.7 – 99.7)KΩ. There was no difference in movement artefact in transport by road vs. air.
Conclusion(s): Neonatal aEEG is feasible and provides readable information during the transport of infants at risk of HIE. The impact of earlier aEEG in this cohort needs to be assessed further.

.jpg)