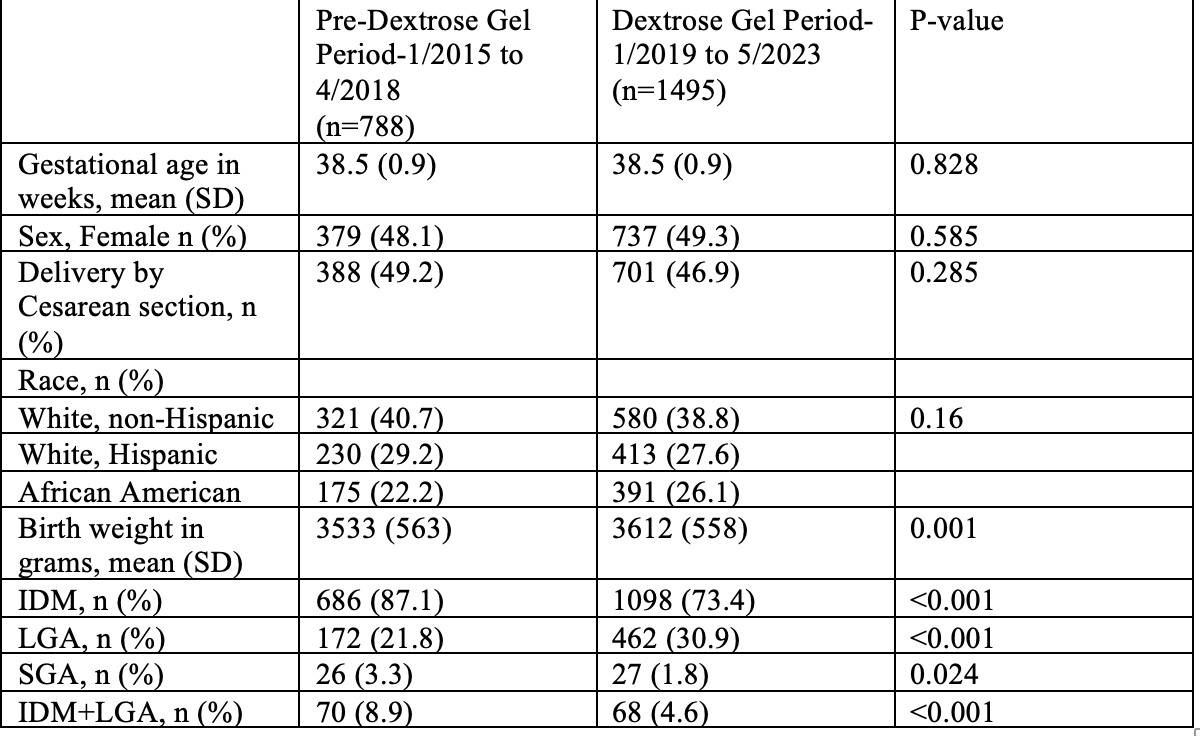
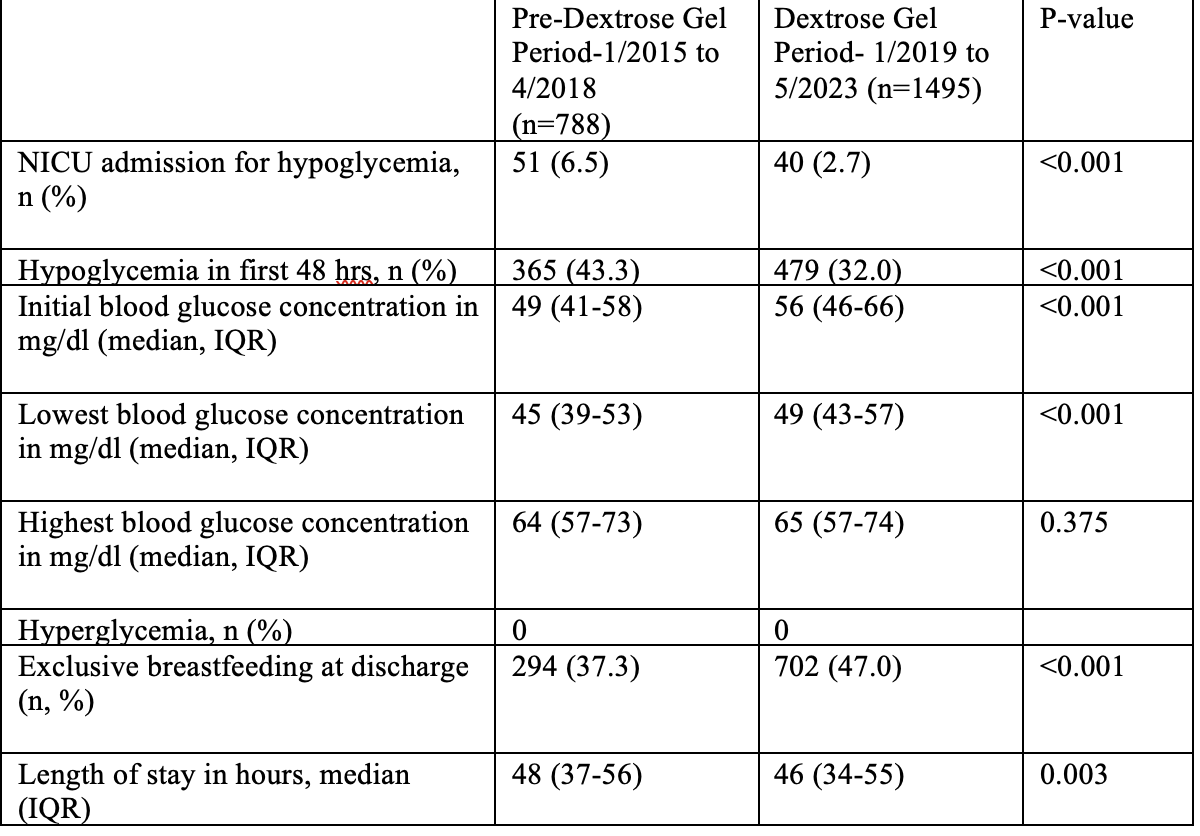
Background: Infants of diabetic mothers (IDM), late preterm infants, large for gestational age (LGA), and small for gestational age (SGA) are at risk of developing pathological hypoglycemia. The use of dextrose gel (DG) for neonatal hypoglycemia in such infants improves outcomes including decreased neonatal intensive care unit (NICU) admission rates. However, DG used prophylactically to prevent hypoglycemia reduced the incidence of hypoglycemia but it did not reduce NICU admissions (Harding et al., hPOD study, PLOS Medicine 2021). At this time, the clinical benefit of prophylactic DG in high-risk newborns is unclear. Objective: The primary objective was to determine if the use of prophylactic DG in infants at risk for hypoglycemia resulted in decreased NICU admissions secondary to hypoglycemia. The secondary objectives were to determine the impact of prophylactic DG on the incidence of hypoglycemia in the first 48 hours, length of stay, and exclusive breastfeeding rates at discharge. Design/Methods: This is a retrospective study of neonates at high risk for hypoglycemia (IDM, LGA, and SGA) born at the University of Arkansas Medical Sciences, Little Rock, AR, between January 2015 and May 2023. The practice of using prophylactic DG (200 mg/kg) started in 05/2018. These high-risk newborns are given buccal DG following their initial feed in the first hour of life, and a blood glucose level is checked 30 minutes later. Late-preterm infants were not included in this practice change. Infants are categorized into two groups for analysis. 1. Pre- dextrose gel (01/2015 to 04/2018) and 2. Dextrose gel (01/2019 to 05/2023). Outcome variables, measured on a continuum and met parametric assumptions, were analyzed by t-tests. Nonparametric, continuous outcomes were analyzed by Wilcoxon's rank-sum test. Categorical variables were assessed by chi-square tests. Results: The two groups had no significant difference in gestational age. Birth weight was greater in the DG group. There was a greater proportion of IDM in the pre-DG group. The use of prophylactic DG resulted in decreased admission rates to the NICU secondary to hypoglycemia, reduced incidence of hypoglycemia in the first 48 hours, and higher initial blood glucose concentration. There was also increased exclusive breastfeeding and decreased length of stay noted with the use of DG. Hyperglycemia was not recorded in either group.
Conclusion(s): The use of prophylactic DG in certain high-risk newborns leads to improved patient outcomes. Without any noted adverse events, we recommend nursery units consider its use to decrease NICU admissions and improve mother-baby bonding.

 photo")