Resident Mayo Clinic Children's Center Rochester, Minnesota, United States
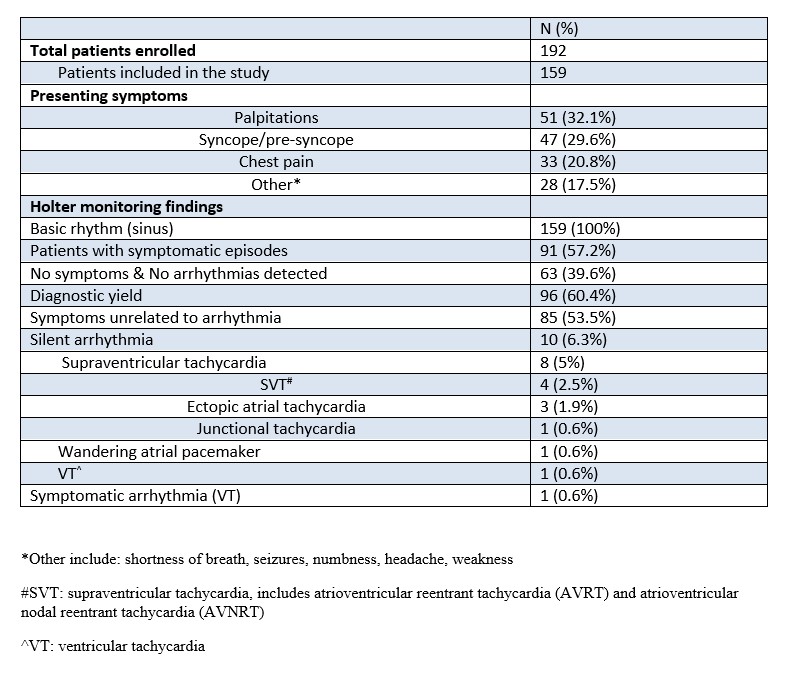
Background: Pediatric patients presenting to an Emergency Department (ED) with symptoms that may represent cardiac arrhythmia can be challenging due to their low-risk nature and variable ability to detect and report symptoms. Although the diagnostic and monitoring utility of Holter Monitors (HM) in adults has been well established, the diagnostic yield and feasibility of HM use in pediatric patients presenting to the ED is not well understood. Objective: We aimed to determine the overall diagnostic yield of HM in pediatric patients presenting to the ED with symptomology suggestive of possible cardiac arrhythmia after a benign screening electrocardiogram (ECG). Design/Methods: We performed a retrospective cohort study of patients ≤ 18 years of age presenting to an academic tertiary care center between January 2015-June 2023 with symptoms suggestive of cardiac arrhythmia who were discharged with a HM after ED evaluation. Patients with a known cardiac history or an abnormal ECG at presentation were excluded. Positive diagnostic yield for the HM was defined as either capture of patient’s reported symptoms while wearing the HM or detection of a silent arrhythmia. Results: There were 192 patients enrolled in the study. Thirty-three patients with a known cardiac history and one patient with an abnormal ECG were excluded. The most common presenting symptoms were palpitations (n=51, 32.1%), followed by syncope/pre-syncope (n=47, 29.6%), and chest pain (n= 33, 20.8%). HM were worn for a median duration of 24 hours. Ninety-one (57.2%) patients reported symptoms while wearing the monitor. The rhythm was sinus or sinus tachycardia in all cases. HM recorded significant “silent” arrhythmias in 10 (6.3%) patients. The most common silent arrhythmia was supraventricular tachycardia (n=8). One patient had symptomatic ventricular tachycardia. The overall diagnostic yield for HM in our study cohort was 60.4%. There were no deaths or other serious adverse events reported in the study cohort.
Conclusion(s): Ambulatory (Holter) monitoring in low risk pediatric patients presenting to the ED with symptoms suggestive of cardiac arrhythmia is a useful diagnostic tool in confirming or excluding arrhythmias. It can provide reassurance for patients and care providers if there is no correlation of reported symptoms with arrhythmias. In addition, a significant subset of patients will have potentially relevant silent arrhythmia detected.