Professor of Pediatrics Stanford University School of Medicine Palo Alto, California, United States
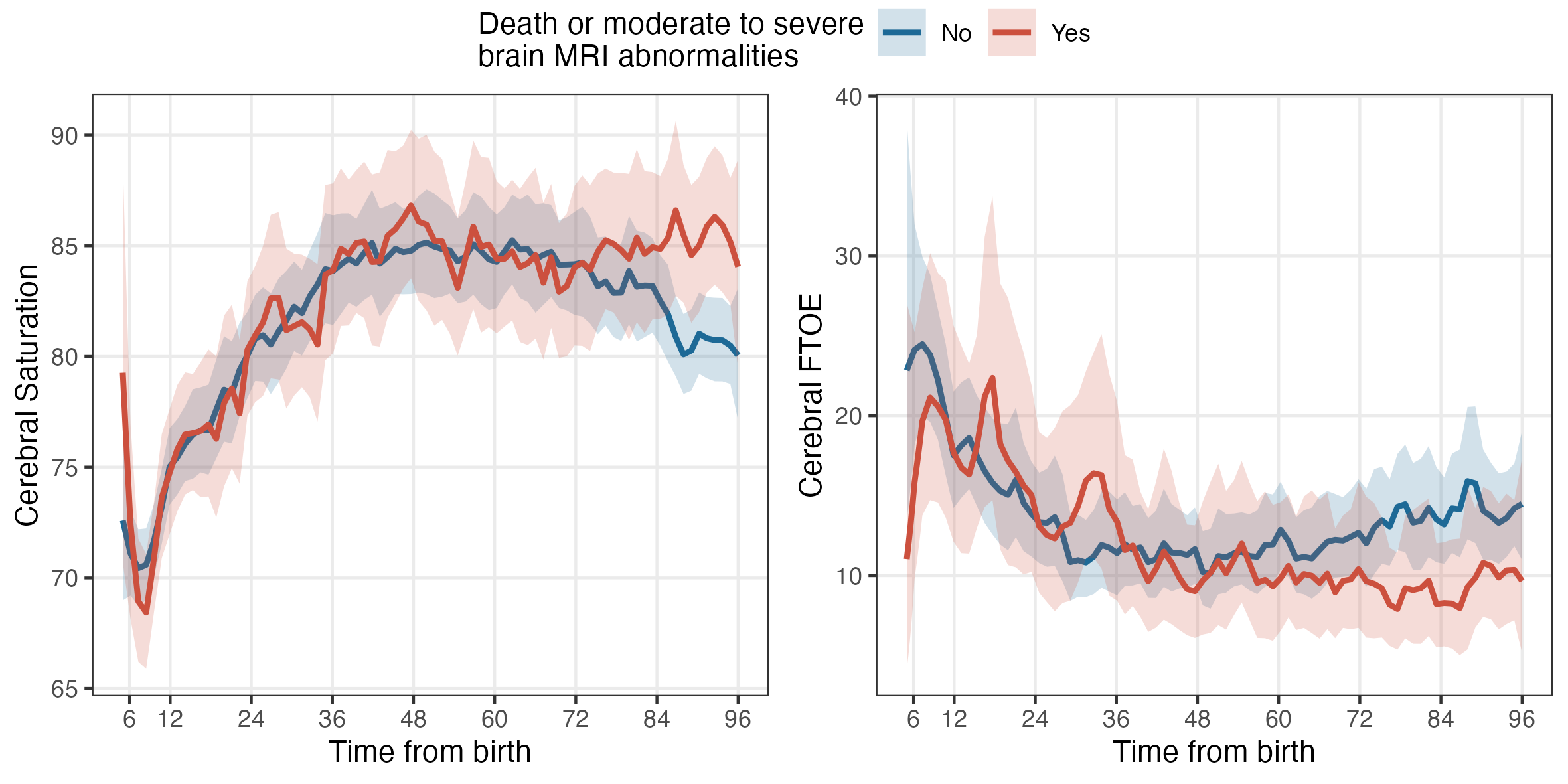
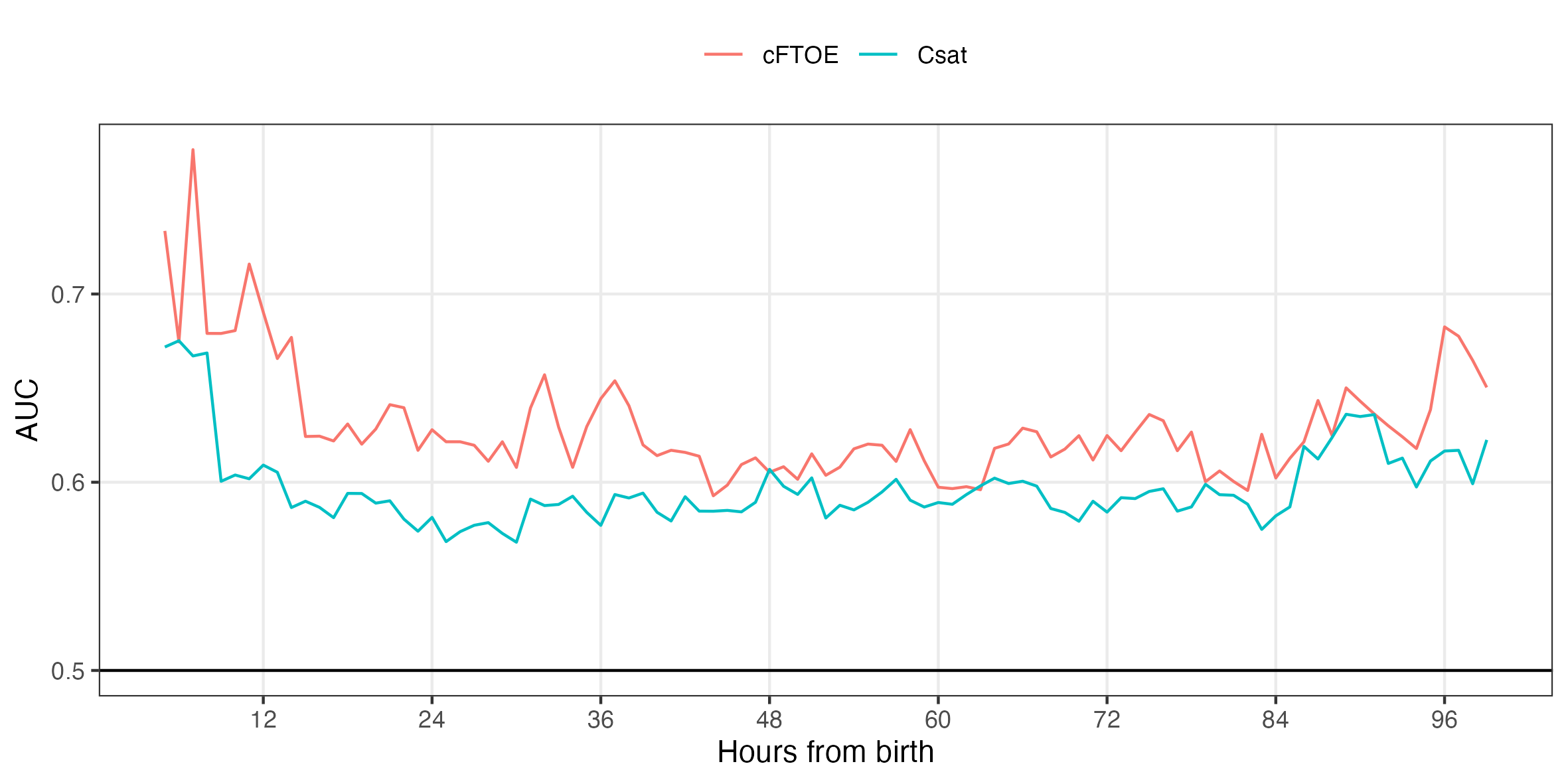
Background: Cerebral oxygenation measures using near-infrared spectroscopy (NIRS) may be associated with adverse outcomes in infants with hypoxic ischemic encephalopathy (HIE) undergoing whole body cooling. However, the time period of monitoring most predictive of outcomes remains unclear. Objective: For term infants with HIE enrolled in the High-Dose Erythropoietin for Asphyxia and Encephalopathy (HEAL) trial, the predictive ability of cerebral oxygen saturation (Csat) and cerebral fractional tissue oxygen extraction (cFTOE) for death or moderate to severe brain magnetic resonance imaging (MRI) injury was investigated. Death or neurodevelopmental impairment (NDI) was explored as a secondary outcome. Design/Methods: Eight centers participating in the HEAL trial utilized cerebral NIRS monitoring for enrolled infants during 72h of whole body cooling and through rewarming using a neonatal sensor applied to the forehead. Brain MRI was obtained on day 4-5 and severity of injury classified by a validated MRI HIE scoring system. Mann-Whitney U test examined differences in Csat and cFTOE averaged over 1h time intervals in the first 96h for infants with and without the primary outcome of death or moderate to severe brain MRI injury. Mean area under receiver operating characteristic curves (AUC) were obtained over 50 splits of training and testing data at these time points. Cerebral NIRS measures as a predictor for the secondary outcome of death or any degree of NDI at 22 to 36 months of age was also explored. Results: 96 infants were enrolled in the NIRS HEAL ancillary study. Death or moderate to severe brain MRI injury occurred in 33 infants (36%); 34 (38%) died or survived with NDI. Infants with the adverse primary outcome had a higher Csat and lower cFTOE both at early time points ( < 6h) and after rewarming (72-96h) (Fig. 1). For optimal prediction of death or moderate to severe brain MRI injury by Csat, AUC was 0.71 at 6h and 0.66 at 96h. With cFTOE as a predictor, AUC was 0.76 at 6h and 0.70 at 96h (Fig. 2). For the secondary outcome of death or NDI, prediction was optimal with cFTOE, resulting in AUC 0.67 at 6h and 0.68 at 96h (Fig. 3). Exposure to erythropoietin did not significantly change cerebral NIRS measures compared to placebo.
Conclusion(s): Cerebral NIRS measures, specifically decreased cFTOE, may predict adverse outcomes in infants with HIE, although early monitoring by 6h after birth or later monitoring by 96h may be most predictive. It is unclear to what degree the depression of cerebral metabolic rate during cooling itself may have impacted predictive ability of NIRS measures during this time period.

 photo")
.png)