Medical Student The Hospital for Sick Children Toronto, Ontario, Canada
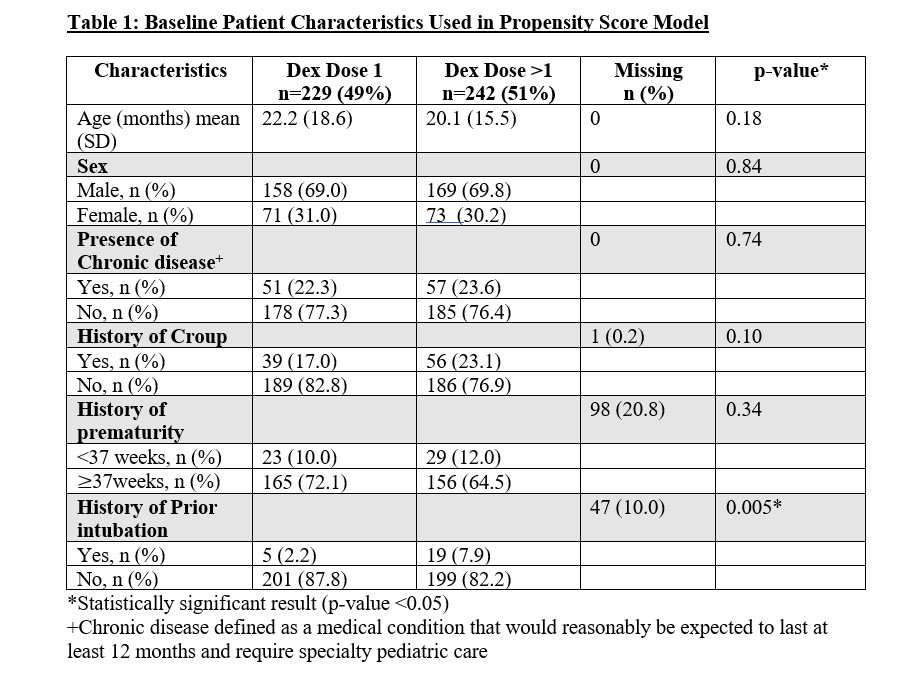
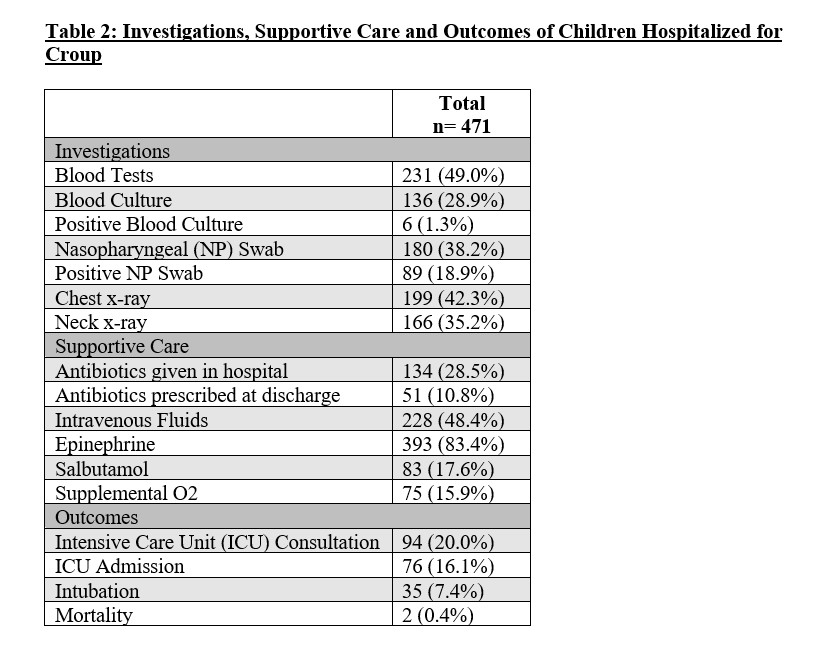
Background: Croup affects approximately 3% of children per year and accounts for 7% of hospitalizations in children < 5 years old. Randomized controlled trial (RCT) evidence supports treating ambulatory children with croup using a single dose of dexamethasone. However, there is a lack of evidence guiding management and describing practice variation for children hospitalized with croup. Objective: To evaluate the association between dexamethasone treatment regime (1 vs >1 dose) and: (i) hospital length of stay (LOS) and (ii) 30-day return to emergency department (ED) visits among children hospitalized with croup. We also describe diagnostic testing, supportive care, and outcomes. Design/Methods: A retrospective cohort study of children hospitalized with croup at a pediatric hospital between 2010-2022. Children < 10 years old, without known airway anomalies and who received dexamethasone were included. Descriptive statistics were used to summarize diagnostic testing, supportive care, and outcomes. Children who received 1 dose vs >1 dose of dexamethasone were compared. Their characteristics were compared using chi-square test and t-test. Logistic regression was used to model patients’ age, sex, and history of prematurity, chronic disease, croup, and intubation as predictors for propensity to receive 1 dose vs >1 dose of dexamethasone. Treatment groups were balanced using inverse probability of treatment weighting. Outcomes included hospital LOS and 30-day return to ED. Results: A total of 471 children hospitalized with croup were included; 229 (49%) received 1 dose of dexamethasone and 242 (51%) received >1 dose. Univariate analysis showed LOS was 54.1 hours longer (95% CI: 40.3-68.0, p= < 0.0001) among those that received >1 dose of dexamethasone; no difference in 30-day return to ED visit (OR 1.3; 95% CI: 0.76-2.2, p=0.33). Table 1 reports characteristics used in the propensity score model. Propensity-weighted analysis demonstrates that patients receiving >1 dose of dexamethasone had a LOS of 52 hours longer (37.5-66.6, p< 0.001) than those who received 1 dose; and no increased odds of 30-day return to ED between the two groups (OR 1.5; 95% CI: 0.97-2.21; p=0.07). Table 2 outlines the proportions of patients with specific diagnostic tests, supportive care, and outcomes.
Conclusion(s): In children hospitalized for croup, the use of multiple doses of dexamethasone was associated with increased LOS; however, no difference in 30-day return to ED. The association between treatment group and LOS may be explained by residual confounding. RCTs are needed to determine optimal dexamethasone treatment regime for inpatient croup.

 photo")